
Quick answer: does the thyroid cause hair loss?
Yes. Both an underactive thyroid (hypothyroidism) and an overactive thyroid (hyperthyroidism) can trigger hair loss, because the thyroid hormones T3 and T4 directly control the hair cycle. The loss is typically diffuse, meaning an even thinning across the whole scalp without bald patches (telogen effluvium). Hair loss occurs in roughly 30% of newly diagnosed overt cases of an underactive thyroid (American Thyroid Association). Once the thyroid is brought back to normal levels (euthyroidism), the hair usually grows back over several months.
- The loss is diffuse across the whole scalp, not patchy.
- There is no fixed TSH value at which the hair starts to fall out.
- Once euthyroidism is reached, the loss is usually reversible.
When the hair starts to thin and at the same time fatigue, weight changes or sensitivity to cold appear, the thyroid quickly comes under suspicion. Rightly so: thyroid hormones are among the strongest control signals for hair growth. This article explains the exact mechanism, sets out how an underactive and overactive thyroid as well as Hashimoto’s fit in, clears up the confusing shedding after starting levothyroxine, and shows which values you should really have measured. Research as of June 2026.
Summary
- How the thyroid controls hair growth
- Underactive thyroid (hypothyroidism) and hair loss
- Overactive thyroid (hyperthyroidism) and hair loss
- Does the thyroid change the hair structure?
- Hashimoto’s thyroiditis and how to distinguish it from alopecia areata
- Hair loss since starting levothyroxine: what lies behind the shedding
- Diagnosis: which thyroid values to have measured for hair loss?
- Treatment and hair regrowth in thyroid hair loss
- Diffuse thyroid hair loss or genetic hair loss?
- Frequently asked questions about hair loss and the thyroid
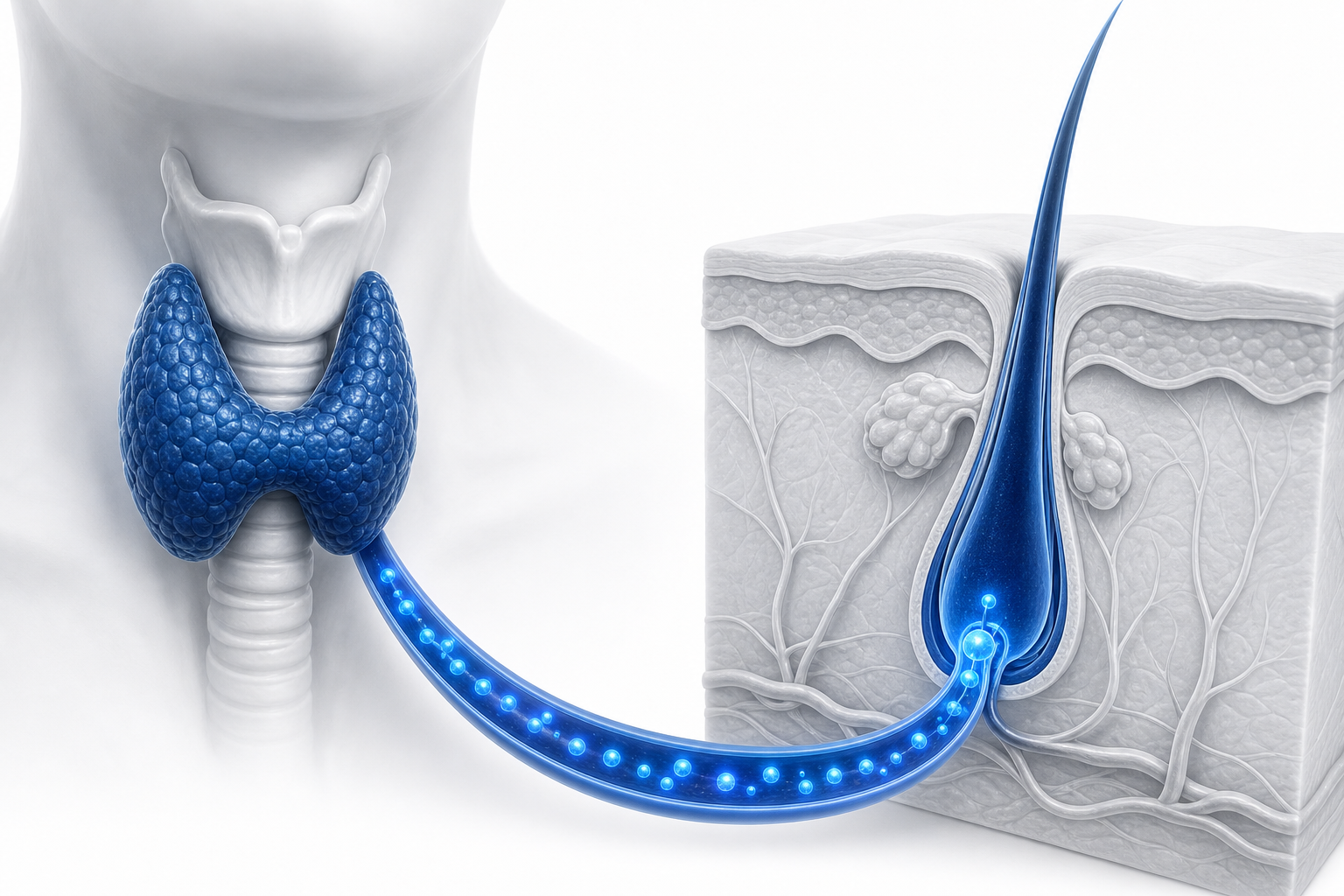
How the thyroid controls hair growth
The thyroid controls hair growth because the hair follicles carry their own thyroid hormone receptors and process thyroid hormone locally. Billoni et al. demonstrated in the British Journal of Dermatology (2000) that the human hair follicle expresses thyroid hormone receptors, with the TRβ1 isoform dominating. The hair therefore responds not only indirectly through the metabolism, but directly to the hormone.
The key study on this comes from van Beek et al. (Journal of Clinical Endocrinology & Metabolism, 2008). T4 prolongs the growth phase (anagen) of the hair follicles in vitro, increases the division of the hair matrix cells and promotes pigmentation. Notably, the follicle transcribes the deiodinase genes D2 and D3 and thereby converts T4 into the more active T3 on site itself.
Put simply: without the right amount of thyroid hormone at the hair root, the hair switches too early from growth mode into the shedding mode. The chain of action in brief: T4 enters the follicle, the enzyme D2 forms T3 from it locally, this binds to the TRβ1 receptor and throttles the anagen inhibitor TGF-β2. As a result, the growth phase stays active for longer. If the hormone balance tips in deficiency or excess, this reverses: the follicles slip prematurely into the resting phase (telogen) and the hair falls out diffusely. How the individual phases interact is explained in our article on the hair growth cycle.
The effect also shows up at the stem-cell level: in the mouse model, switching off the receptors TRα1 and TRβ blocks the mobilisation of hair follicle stem cells out of the resting phase, mediated by a disrupted Wnt/β-catenin pathway (Contreras-Jurado et al., 2015). This explains why a thyroid disorder does not merely slow the supply of new hairs but throws the whole cycle out of sync. It is precisely this shared timing of many follicles that is the reason the loss appears diffusely across the whole scalp rather than in individual patches.
Underactive thyroid (hypothyroidism) and hair loss
An underactive thyroid causes diffuse hair loss: an even thinning across the whole scalp without bald patches. In Germany, overt hypothyroidism affects about 1% of the population, while the latent (subclinical) form ranges from 3 to 16% depending on age and measurement method (IQWiG, gesundheitsinformation.de). The often-quoted figure of 5 in 100 of those affected combines both forms.
Typical for the hair in an underactive thyroid, alongside the thinning, is dry, brittle hair as well as a possible loss of eyebrow and body hair (Cleveland Clinic). A classic sign is the so-called Hertoghe sign, the loss of the outer third of the eyebrows. However, it is non-specific and on its own is not proof, more on that in the FAQ section.
Fatigue, weight gain, sensitivity to cold and dry skin often occur alongside it (NHS). For the GP assessment of an abnormal value, the German AWMF S2k guideline 053-046 “Raised TSH value in the GP practice” (DEGAM, as of 19/01/2024) is the authoritative reference. We cover an underactive thyroid in more depth in our detailed article on hair loss caused by hypothyroidism.

Overactive thyroid (hyperthyroidism) and hair loss
An overactive thyroid also causes diffuse, non-scarring hair loss. The hair often looks fine, soft and silky, is less able to withstand tension and breaks more easily. The outer third of the eyebrows, the eyelashes as well as the underarm and pubic hair can also be affected (NIH/PMC review “Impact of Thyroid Dysfunction on Hair Disorders”).
The mechanism is, in a sense, the mirror image of the underactive thyroid: an excess of T3 and T4 shortens the growth phase and accelerates the transition into the telogen phase, and on top of that oxidative stress damages the follicles. Accompanying symptoms are typically increased sweating, weight loss, a racing heart and inner restlessness.
On frequency, the figure circulates that hair loss affects up to 15% of patients with an overactive thyroid (Deutsches Schilddrüsenzentrum). This number comes from a secondary source and should be understood as a rough guide. What matters is the message behind it: not only too little but also too much thyroid hormone costs hair.
In practice this means an overactive thyroid is easily overlooked when searching for the cause, because many people first think only of an underactive one. Anyone who notices fine, brittle hair together with a racing heart, restlessness and unexplained weight loss should have an overactive thyroid specifically investigated. Here too the rule applies: first treat the functional disorder, then the hair cycle usually recovers over several months.
Does the thyroid change the hair structure?
Yes, a thyroid disorder often changes the hair structure itself, not just the density. With an underactive thyroid the hair typically becomes dry, brittle, fragile and looks straw-like to wiry (NIH/PMC review; Cleveland Clinic). Many of those affected notice the change in texture earlier than the actual loss.
With an overactive thyroid the opposite shows: the hair becomes fine, soft and silky, with some describing it as fluffy hair that holds barely any shape (NIH/PMC review). This change in texture is a practical clue for your own assessment. It remains an indication, though, not proof. Only the blood test provides certainty.
Hashimoto’s thyroiditis and how to distinguish it from alopecia areata
Hashimoto’s thyroiditis is the most common cause of an underactive thyroid and is an autoimmune disease. Diagnostically, it usually shows a rise in TPO antibodies (antibodies against thyroid peroxidase), occasionally also Tg antibodies. The hair loss here follows the diffuse pattern of an underactive thyroid.
It is important to distinguish it from alopecia areata, patchy hair loss. Both autoimmune processes occur together more frequently: a population-based case-control study with 33,401 affected individuals (Wohl et al., JDDG 2026) found an odds ratio of 1.67 (95% confidence interval 1.58 to 1.77) for the association between Hashimoto’s and alopecia areata. A Mendelian randomisation (Frontiers in Endocrinology, 2024) supports a causal indication from hypothyroidism to alopecia areata (OR 1.43), but not from an overactive thyroid.
The key point for those affected: alopecia areata is a different disease from thyroid hair loss. It runs a patchy course, with coin-sized, sharply demarcated bald patches, and is based on a T-cell attack on the follicle. Simply normalising the TSH does not cure alopecia areata. So anyone who, alongside diffuse thinning, suddenly discovers round bald spots should have this assessed separately by a dermatologist.
| Feature | Thyroid hair loss (telogen effluvium) | Alopecia areata (patchy hair loss) |
|---|---|---|
| Pattern | diffuse, whole scalp | patchy, round sharply demarcated patches |
| Cause | hormone deficiency or excess shifts the hair cycle | autoimmune T-cell attack on the follicle |
| Response to thyroid treatment | usually resolves after euthyroidism | not cured by normalising TSH |
Special case after pregnancy (postpartum thyroiditis)
Not every instance of hair loss after birth is the normal postpartum hair loss that resolves on its own. Behind it can also lie a temporary inflammation of the thyroid after birth, postpartum thyroiditis. It often runs through a phase with an overactive thyroid followed by an underactive one and can shift the hair cycle in the same way. If the hair loss after pregnancy is unusually heavy or persists beyond the usual time, the thyroid values should be checked by a doctor.
Hair loss since starting levothyroxine: what lies behind the shedding
Hair loss directly after starting or adjusting the dose of levothyroxine is a frequently described phenomenon and at first seems paradoxical. The explanation: many follicles that were stuck in the resting phase are reactivated at the same time (telogen release) and push out their old hairs all at once. A second possible reason is a dose that is not yet correctly adjusted, meaning either a persisting underactive thyroid or a temporary overactive one.
This shedding usually begins a few months after the start, because the follicles react with a delay, and it generally lasts only a few months. As the TSH value stabilises it usually subsides. The evidence for this comes predominantly from patient and pharmaceutical information portals (such as Paloma Health, Drugs.com), not from hard primary literature. Precise figures in weeks would therefore be unreliable.
Important context
Do not stop levothyroxine on your own in the event of such shedding. The flare-up is usually temporary, and stopping would worsen the underlying underactive thyroid. The hairs falling out during this phase are not lost permanently; they are making way for new, healthy hair. Discuss what you have observed with your doctor and wait for the correct dose to be set.
Diagnosis: which thyroid values to have measured for hair loss?
The work-up of hair loss caused by the thyroid includes the baseline value TSH as well as the free hormones fT3 and fT4, supplemented by the antibodies TPO-Ab and, where Graves’ disease is suspected, TRAb. An important note first: all reference ranges are laboratory- and method-dependent, so they only apply “depending on the lab”. And the units mU/L, mIU/L and µIU/ml are 1:1 identical, even though they are written differently on reports.
The aha moment when reading the report: TSH behaves inversely to fT3 and fT4. With an underactive thyroid the TSH is raised, while fT3 and fT4 are low. With an overactive thyroid it is the other way round. This is due to the feedback loop between the pituitary gland and the thyroid, in which the TSH, as the control hormone of the pituitary, drives the thyroid. A sonography (ultrasound of the thyroid) can additionally be useful.
The antibodies separate the causes from one another: raised TPO-Ab point to Hashimoto’s thyroiditis, while a positive TRAb suggests Graves’ disease and usually stays negative in pure Hashimoto’s. The TPO-Ab cut-off is strongly assay-dependent and ranges, depending on the lab, from around 9 to 60 IU/ml, which is why a single numerical value without the reference range of the respective lab says little. This is exactly why every report should carry the lab’s own normal range, which is what you orient yourself by.
| Value | Underactive | Normal range | Overactive | Unit |
|---|---|---|---|---|
| TSH | raised (above approx. 4.2) | 0.27–4.20 | lowered (below approx. 0.27) | µIU/ml (= mIU/L = mU/L) |
| fT4 (free T4) | lowered | 0.8–1.8 | raised | ng/dl |
| fT3 (free T3) | lowered | 2.0–4.4 | raised | pg/ml |
| TPO-Ab | raised in Hashimoto’s | below 34 (negative) | usually normal | IU/ml |
| TRAb | usually normal | below 1.0 (negative) | raised in Graves’ | mU/l (= IU/L) |
Reference ranges vary by laboratory and measurement method. The TPO-Ab cut-off lies between around 9 and 60 IU/ml depending on the assay; 34 IU/ml is a common German lab value. Sources: Endokrinologikum Hamburg, Deutsches Schilddrüsenzentrum.
If the GP has only measured the TSH and the hair keeps falling out, it is worth a targeted visit to an endocrinologist with a clear list of values. You can print out the following checklist or take it as a screenshot. The role blood values play in hair loss generally is something our article on the blood test for hair loss explores in more depth.
Endocrinologist briefing: values to take with you
Request these values from the endocrinologist if only the TSH was determined and the hair keeps falling out:
- ☐ fT3 (free T3) – thyroid function
- ☐ fT4 (free T4) – thyroid function
- ☐ TPO-Ab – autoimmune marker (Hashimoto’s)
- ☐ TRAb – autoimmune marker (Graves’ disease)
- ☐ Ferritin – iron stores, a common contributing cause of diffuse hair loss
- ☐ Vitamin D (25-OH) – a common deficiency
- ☐ Selenium – only in the Hashimoto’s context and where a deficiency has been confirmed, under medical supervision
No self-diagnosis: this list is a basis for the conversation at your doctor’s appointment, not a substitute for medical assessment.
Treatment and hair regrowth in thyroid hair loss
The treatment of thyroid hair loss consists of correcting the underlying functional disorder, not treating the hair separately. With an underactive thyroid, levothyroxine replaces the missing T4. After a dose change the TSH is usually checked every 6 to 8 weeks (NHS). Once euthyroidism is reached, the hair cycle usually normalises on its own.
With an overactive thyroid, antithyroid drugs throttle the hormone production. The telogen effluvium then usually resolves over several months (NIH/PMC review). In both cases the rule applies: normalising the telogen rate takes time, because the resting phase of the affected follicles has to run its course first before new hairs push through.
How long this takes can only be given as a rough guide. A visible improvement typically shows in the region of 3 to 6 months after normalisation, full density may only be reached after 9 to 12 months, and with a long prior illness even later (Forum Schilddrüse). The timeline below shows the usual pattern.
| Period | What happens in the follicle |
|---|---|
| Month 1–2 | The hormone level normalises, the loss slowly stops. |
| Month 3–4 | The follicles re-enter the growth phase (anagen). |
| Month 5–6 | The first new, still thin hairs (baby hair) become visible. |
Rough guide. The period of 3 to 6 months corresponds roughly to the length of the telogen phase before new hairs push through.
A practical reassurance: normal washing, combing or colouring does not speed up the loss. The affected hairs are already in the telogen phase and would come away anyway; the daily handling only brings them into view a little sooner, rather than costing additional hairs.
Selenium in Hashimoto’s: what the evidence really shows
Selenium is often touted in the Hashimoto’s context as a supplement, but the evidence for it is weak and inconsistent. A Cochrane review (van Zuuren et al., 4 randomised trials, 463 participants) states verbatim that the data on selenium supplementation in Hashimoto’s is “incomplete and not reliable”, that is, too incomplete and unreliable for clinical decisions. Individual studies showed a reduction in TPO-Ab, but their clinical significance remains unclear.
A more recent meta-analysis from 2024 (35 studies) also sees a TPO-Ab reduction, but with low quality of evidence and strong heterogeneity (I² = 90%). No general recommendation can be derived from this. Selenium comes into question at most where a deficiency has been confirmed and under medical supervision, not as a standard therapy and not on your own initiative. Which nutrients make sense and when is something our article on supplements for hair loss sets out.
Diffuse thyroid hair loss or genetic hair loss?
Thyroid hair loss is diffuse and affects the whole scalp, whereas genetic (androgenetic) hair loss follows a pattern: a receding hairline and thinning crown in men, a widening parting in women. The mechanism is fundamentally different: a shift in the hair cycle through hormone deficiency on the one hand, a DHT-mediated miniaturisation of the follicles on the other.
| Feature | Thyroid (telogen effluvium) | Androgenetic alopecia (AGA) |
|---|---|---|
| Pattern | diffuse, whole scalp | receding hairline and crown (men), widening parting (women) |
| Mechanism | shift of the hair cycle into the telogen phase | DHT-mediated follicle miniaturisation |
| Reversibility | usually reversible after euthyroidism | progressive, not reversible without treatment |
Both can be present at the same time, and that is not uncommon. In a study of women with androgenetic alopecia, 31.25% also had hypothyroidism (NIH/PMC review). A Mendelian randomisation, however, showed no causal link from the thyroid to androgenetic alopecia (p above 0.05). The two causes are independent and can overlap. You can read more about the pattern type under androgenetic alopecia.
For practice this means: the first step is to find out which type is present. Diffuse thyroid or TE hair loss should be treated by a physician and is not suitable for a hair transplant. Only genetic, pattern hair loss responds to hair growth products or a hair transplant.
To clarify whether you even have genetic (pattern) hair loss that a treatment can target, the free Elithair hair analysis helps. It cannot assess the thyroid status itself. That must be clarified by a doctor through a blood test.
Frequently asked questions about hair loss and the thyroid
Which TSH value causes hair loss?
There is no fixed TSH threshold for hair loss. The American Thyroid Association expressly states that there is no reliable relationship between the level of TSH, T3 or T4 and the severity of symptoms. Hair loss can occur even with a subclinical underactive thyroid. A single cut-off therefore cannot be given responsibly.
Does the hair grow back after the thyroid is treated?
Usually yes. After euthyroidism is reached, the hair cycle generally recovers over several months, with a visible improvement often showing after 3 to 6 months. Full density may take longer.
Hashimoto’s and hair loss: what to do?
Have the thyroid treated by a doctor (usually levothyroxine) and, alongside the TSH, have the TPO-Ab as well as accompanying values checked. If round, sharply demarcated bald spots also appear, you should think of alopecia areata. That is a separate disease that is treated separately.
Can an overactive thyroid also cause hair loss?
Yes. An overactive thyroid also triggers diffuse hair loss, often with finer, softer hair that breaks more easily (NIH/PMC review). After the overactive thyroid is treated, the hair loss usually resolves over months.
Do you lose eyebrows because of the thyroid?
A loss of the outer (lateral) third of the eyebrows is possible, the so-called Hertoghe sign. It is considered classic but is non-specific and also occurs in atopic dermatitis and other conditions. On its own it is not proof of a thyroid disorder (DocCheck Flexikon; QJM Oxford 2023).
Hair loss since starting the thyroid tablets: is that normal?
An initial shedding at the start of levothyroxine therapy is frequently described and usually temporary. Do not stop the tablets on your own; discuss what you have observed with your doctor and wait for the correct dose to be set.
How long does regrowth take?
3 to 6 months until a visible improvement appears. Full density may only be reached after 9 to 12 months or later, because the hair cycle first has to catch up on the telogen phase it has been through.
Scientific sources
- van Beek N et al.: Thyroid hormones directly alter human hair follicle functions. J Clin Endocrinol Metab (2008). PubMed
- Billoni N et al.: Thyroid hormone receptor beta1 is expressed in the human hair follicle. Br J Dermatol (2000). PubMed
- Wohl Y et al.: Association of Hashimoto’s thyroiditis and alopecia areata (OR 1.67). JDDG (2026). Wiley Online Library
- van Zuuren EJ et al.: Selenium supplementation for Hashimoto’s thyroiditis (Cochrane review). Cochrane Database Syst Rev (2013). PubMed
- Hussein RS et al.: Impact of Thyroid Dysfunction on Hair Disorders (review). NIH/PMC (2023). PMC
- American Thyroid Association: Hair loss and thyroid disorders (no fixed TSH threshold). Clinical Thyroidology for Patients. thyroid.org
- DEGAM: AWMF S2k guideline 053-046 “Raised TSH value in the GP practice” (2024). AWMF Register
- IQWiG / gesundheitsinformation.de: Underactive thyroid (hypothyroidism), prevalence data. gesundheitsinformation.de
This article is for information purposes and does not replace a medical diagnosis or treatment. If you experience hair loss and suspect a thyroid disorder, please consult your doctor.
Related topics from our hair loss cluster: vitamins for hair loss, iron deficiency and hair loss as well as the overview of the causes of hair loss. Especially for women, our article on hair loss in women is worth a read, along with the overview of hormones and hair.

Dr. Imad Moustafa
Hair transplant specialist