You have been on Zepbound for a few months, the number on the scales is finally heading down, and just at that moment you start noticing far more hair in your brush each morning. This worry is especially common among people taking Zepbound, and there is a real basis to it. With the active ingredient tirzepatide, Zepbound produces the highest average weight loss of any weight-management medicine approved in the United States. And it is precisely that dramatic, rapid weight loss, rather than the drug itself, that is the true trigger behind the hair loss.
In this article we look at what the clinical SURMOUNT trials and the FDA label actually show, why women on Zepbound are affected fourteen times more often than men, how the hair loss unfolds over time, and what you can practically do about it. We also place Zepbound in context against Mounjaro (the same active ingredient, but licensed for diabetes) and Wegovy (the obesity counterpart from the semaglutide family). This article is for information only and is not a substitute for medical advice. Speak to your treating doctor before making any change to your medication.
Does Zepbound cause hair loss? Yes, Zepbound (tirzepatide) can trigger hair loss. In almost all cases this is a telogen effluvium brought on by the rapid, marked weight loss, rather than by any direct damage to the hair follicles. In the SURMOUNT-1 and SURMOUNT-2 licensing trials, around 5% of those treated reported hair loss, compared with roughly 1% on placebo. The loss is temporary in nearly every case.
In short: does Zepbound cause hair loss?
- Yes, Zepbound (tirzepatide) can trigger hair loss. In the SURMOUNT-1 and SURMOUNT-2 trials, around 5% of those treated reported it, compared with roughly 1% in the placebo group.
- The cause is almost always a telogen effluvium, set off by the rapid weight loss, not by the drug directly damaging the hair follicles.
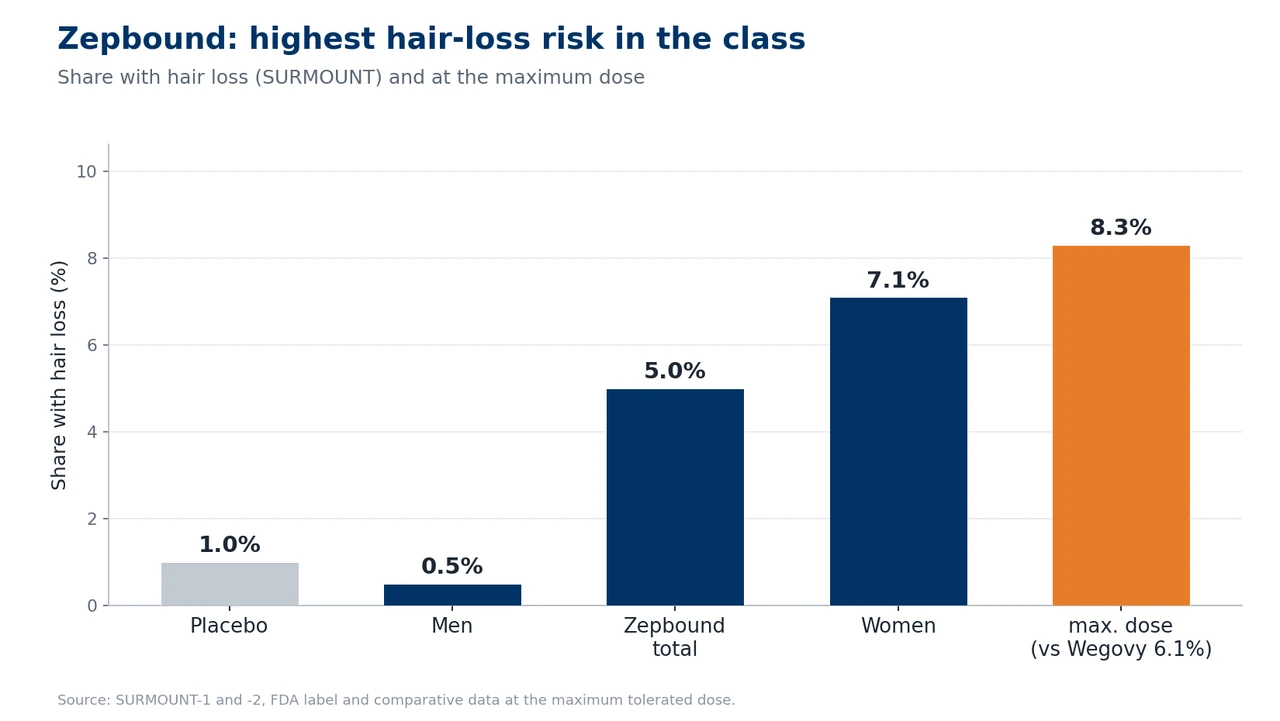
- Women are affected far more than men: 7.1% versus 0.5% according to the FDA label. That is the largest sex difference anywhere in the GLP-1 field.
- The hair loss is temporary and reversible in nearly every case. Regrowth typically begins 6–12 months after the weight has stabilised.
- Because Zepbound achieves the greatest weight loss of the entire drug class, it also carries the highest risk of a telogen effluvium.
If you are losing hair on Zepbound, in the vast majority of cases it is a temporary phenomenon that resolves on its own. A hair transplant is not needed at this stage. The matter only becomes important if, once recovery is complete, a lasting, patterned form of hair loss emerges. That is precisely the distinction we clarify here.
Summary
- Does Zepbound cause hair loss? The clinical evidence
- How does the hair loss on Zepbound present?
- Why does it happen? The mechanism behind Zepbound and hair loss
- Timeline: when does the hair loss start and when does the hair grow back?
- Who is most at risk on Zepbound?
- What exactly is Zepbound?
- The link with hereditary hair loss (AGA)
- Prevention: what you can do while losing weight
- Treatment and regrowth: what really helps
- The Elithair approach: when is a hair transplant appropriate?
- Zepbound compared with other GLP-1 medicines
- When to see your GP or a dermatologist
- Frequently asked questions about Zepbound and hair loss
- Conclusion: does Zepbound cause hair loss?
- Sources
Does Zepbound cause hair loss? The clinical evidence
With Zepbound, hair loss is not speculation from internet forums but an officially documented side effect. In the FDA-approved Prescribing Information (NDA 217806), alopecia is listed explicitly in section 6.1. The basis is the pooled data from the two pivotal licensing trials, SURMOUNT-1 and SURMOUNT-2. Across all dose groups the hair-loss rate was around 5%, compared with roughly 1% on placebo. That equates to an approximately fivefold increase in risk.
The wording in the label itself is decisive. Eli Lilly describes the side effect, in effect, as “hair loss that was associated with the weight reduction”. So it expressly does not say “caused by tirzepatide”; instead the hair loss is attributed to the weight loss. This distinction runs through all the current research and is the key to understanding the topic.
SURMOUNT-1: the figures by dose group
SURMOUNT-1 (published in the New England Journal of Medicine in 2022) studied 2,539 adults with obesity but without type 2 diabetes over 72 weeks. Tellingly, the hair-loss rate did not climb further with higher doses but stayed similar across all of them. That fits neatly with the idea of weight loss as the real driver, because weight loss itself also plateaus beyond a certain dose.
| Group (SURMOUNT-1) | Hair loss | Avg. weight loss |
|---|---|---|
| Tirzepatide 5 mg | 5.1% (32/630) | −15.0% |
| Tirzepatide 10 mg | 5.3% (34/636) | −19.5% |
| Tirzepatide 15 mg | 4.9% (31/630) | −20.9% |
| Placebo | 0.9% (6/643) | −3.1% |
SURMOUNT-5: the head-to-head comparison with Wegovy
SURMOUNT-5 is particularly revealing: a direct head-to-head comparison between Zepbound and Wegovy over 72 weeks. At the maximum tolerated dose, hair loss occurred in 8.3% of people on Zepbound and 6.1% on Wegovy. In parallel, the weight loss on Zepbound was also markedly greater: 20.2% versus 13.7%. This lockstep between greater weight loss and a higher hair-loss rate is the recurring pattern across the whole topic.
FAERS data and meta-analyses
A disproportionality analysis of the FDA’s FAERS reporting database (Godfrey et al., JEADV 2025) found a reporting odds ratio of 1.73 for tirzepatide (95% confidence interval 1.42 to 2.09), and 2.46 for semaglutide. Both signals are statistically significant. Interestingly, the FAERS signal for tirzepatide is lower than for semaglutide, even though the clinical trial rates are higher. One plausible explanation: Zepbound was only approved in November 2023 and is therefore newer, which leads to fewer spontaneous reports in the early phase.
Several systematic reviews confirm the picture. A meta-analysis in Science Progress (Gupta et al., 2026) found a 3.4-fold increased risk of alopecia across 24 studies for users of GLP-1 and GIP drugs, and groups tirzepatide together with semaglutide among the agents with the highest rates. A large real-world cohort of 547,993 matched patients (Vidal/Akiska et al., JAAD International 2026) showed, at 12 months, an increased risk of both telogen effluvium (raised by around 76%) and androgenetic alopecia (raised by around 64%).
How does the hair loss on Zepbound present?
In most cases the hair loss on Zepbound is a telogen effluvium, that is, a diffuse shedding across the whole scalp. You do not lose hair in patches or at one particular spot, but a little everywhere. Instead of the normal 50 to 100 hairs a day, it can suddenly be 200 to 300 or more. You notice it as more hair in the brush, the plughole and on the pillow, as a thinning ponytail, and as a visibly lower density, especially when the hair is wet or in bright light.
The well-known New York dermatologist Dr Marisa Garshick (Weill Cornell Medicine) sums it up: the loss is diffuse, you notice it from all over. That is the central difference from hereditary hair loss, which follows a fixed pattern. Exactly how a hair moves into the resting phase and falls out is explained in detail in our article on the hair growth cycle.
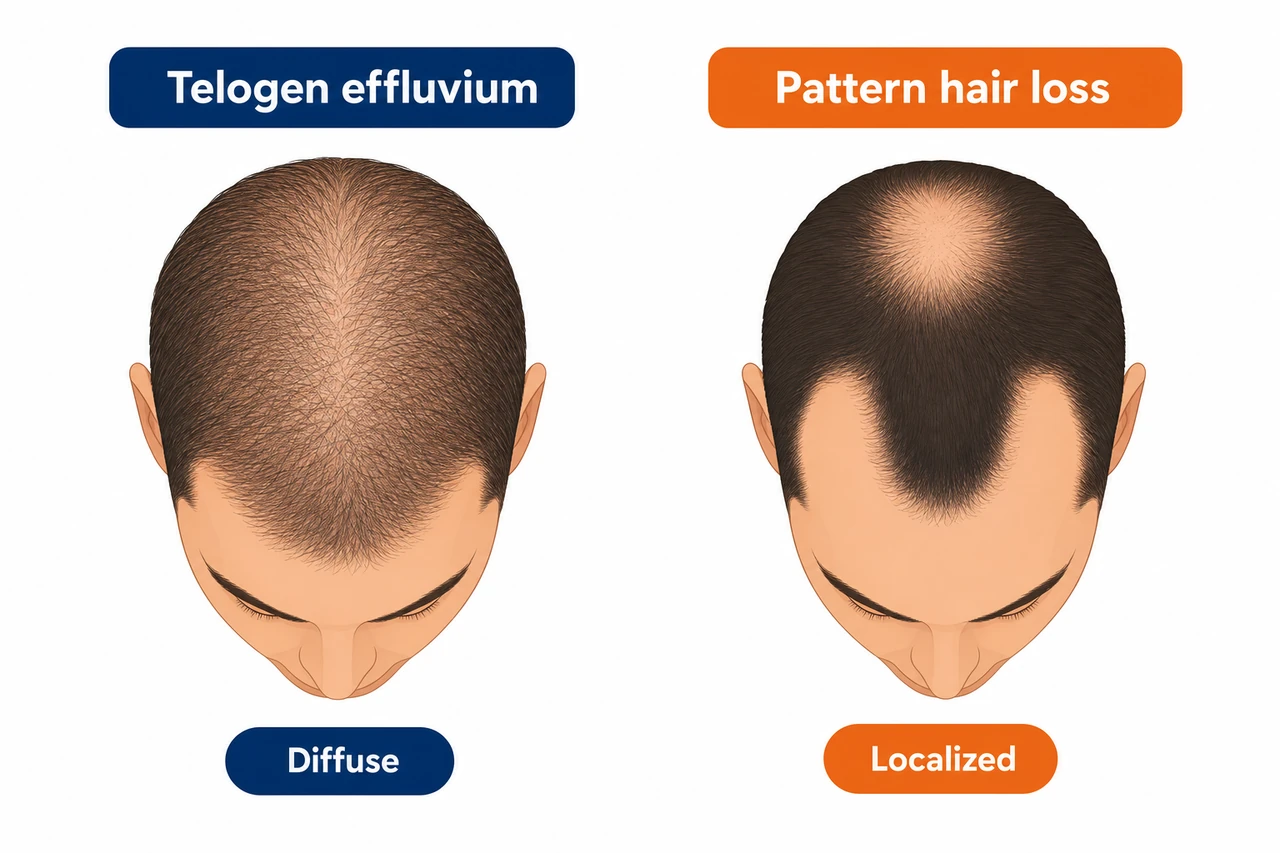
It is important to distinguish this from androgenetic alopecia (AGA), the hereditary form of hair loss. The two can occur at the same time, and a telogen effluvium can unmask a previously invisible AGA. The comparison below will help you tell them apart.
| Feature | Telogen effluvium | Androgenetic alopecia |
|---|---|---|
| Pattern | Diffuse, across the whole scalp | Patterned (receding temples, crown, parting) |
| Course | Acute, begins 2 to 4 months after the trigger | Gradual, progressing over years |
| Reversible? | Yes, almost always completely | No, progresses without treatment |
| Trigger | Rapid weight loss, stress, nutrient deficiency | Genetic predisposition, DHT sensitivity |
Which path is yours? The key fork in the road
Diffuse loss (telogen effluvium): reversible, no hair transplant needed. What helps is patience over 6 to 12 months, enough protein, and a check of your ferritin and iron. If you are unsure, a hair analysis will clarify where you stand.
Patterned loss (receding temples, crown): here the weight loss may have unmasked an already present hereditary alopecia. This is the situation in which a permanent solution becomes worth considering. How to tell the two cases apart reliably, and when a transplant might be appropriate, is covered further down.
Why does it happen? The mechanism behind Zepbound and hair loss
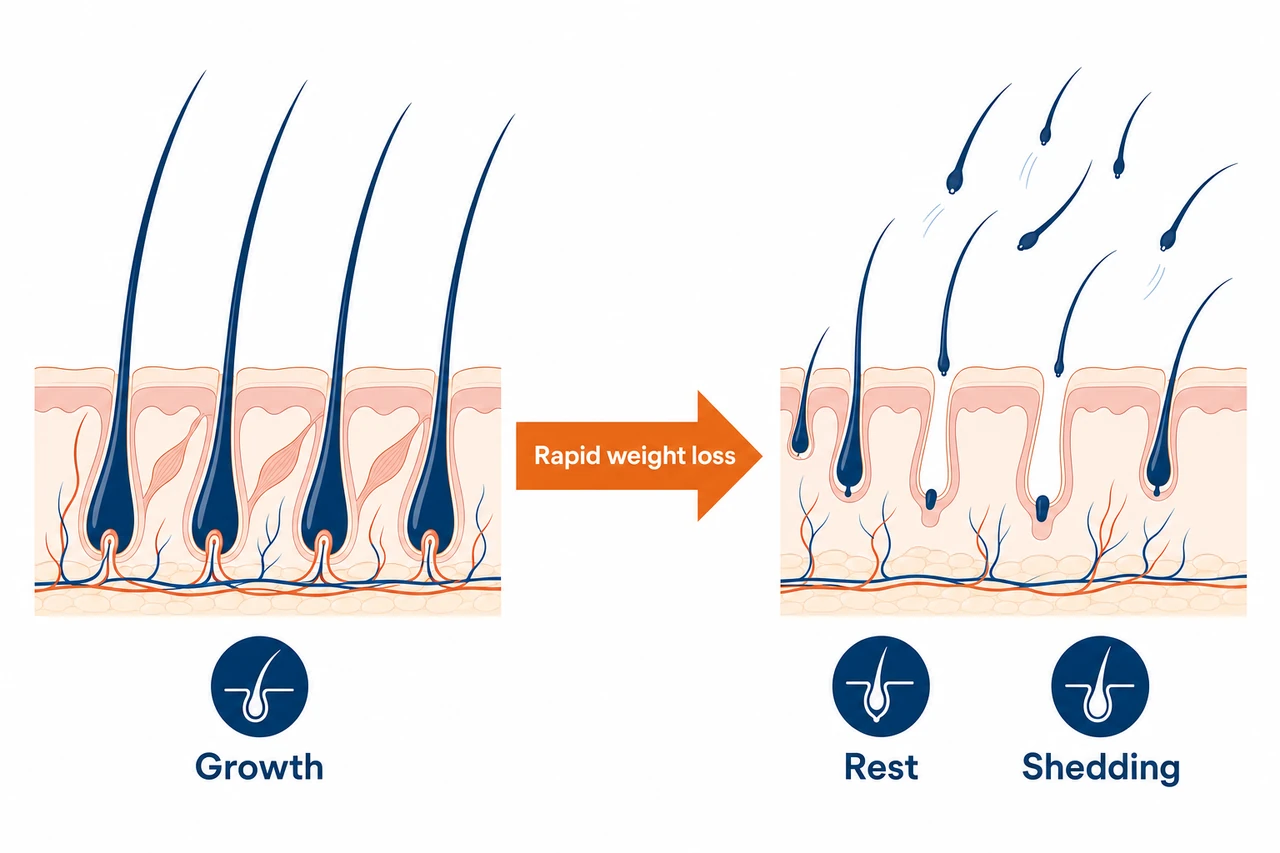
The main mechanism is a telogen effluvium caused by rapid weight loss. And here Zepbound holds an unfortunate special position: with an average of minus 20.9% on 15 mg in SURMOUNT-1, up to minus 22.5% over a longer course and even minus 26.6% in SURMOUNT-3, it achieves the greatest weight loss of any weight-management medicine approved in the US. The more dramatic and rapid the drop in weight, the greater the physiological stress that puts the brakes on hair growth.
The body interprets rapid weight loss as an emergency. It redirects energy and nutrients to the vital organs and dials back hair growth, a function that is not essential for survival. The result: huge numbers of hair follicles switch prematurely from the growth phase (anagen) into the resting phase (telogen). Normally only 5 to 10% of follicles are in the resting phase; under severe stress, up to 70% can enter it at once. Because the resting phase itself lasts two to three months, the hairs only fall out after a delay. That is why the hair loss does not become visible until 2 to 4 months after starting treatment.
Nutrient deficiency amplifies the effect
Zepbound strongly suppresses appetite by activating both GIP and GLP-1 receptors at the same time. When you eat considerably less, you also take in less of the nutrients your hair needs. Three of them are particularly critical:
- Protein. Hair is made up of around 90% keratin. If protein intake drops below 0.8 g per kilogram of body weight a day, the risk of a telogen effluvium doubles.
- Iron and ferritin. Iron is a cofactor for a key enzyme in DNA synthesis within the hair matrix cells. A ferritin level below roughly 24 to 30 ng/mL shortens the growth phase. Women are more vulnerable in any case because of menstruation.
- Zinc. Essential for the proliferation of the skin cells from which hair forms. Studies show significantly lower zinc levels in people with telogen effluvium.
On top of this comes the hormonal side. Marked weight loss activates the stress axis with increased cortisol release, which pushes hair follicles further into the resting phase. Oestrogen levels also change, because fat tissue takes part in hormone production. Just how closely hormones and hair growth are linked is explored in our article on hormones and hair.
The decisive point
No current review has been able to demonstrate direct damage to the hair follicles by tirzepatide. The hair loss is a secondary effect of the weight loss and the accompanying nutrient deficit. On present evidence, tirzepatide has no toxic effect on the hair follicles. That is precisely why the hair usually comes back on its own.
Because tirzepatide is also the active ingredient in Mounjaro, it is worth looking at the mechanism across the indications. The deeper drug-level mechanics can be found on our hub page on tirzepatide and hair loss.
Timeline: when does the hair loss start and when does the hair grow back?
The hair loss on Zepbound follows a predictable timeline. Knowing it takes away a great deal of the panic that many people feel in the first few months.

- Months 0 to 3 (latency). Treatment begins and the weight loss starts, often at its fastest in the first 8 to 12 weeks. The follicles are already switching into the resting phase, but the hairs are still firmly rooted. There is as yet no visible hair loss.
- Months 2 to 4 (onset). The resting hairs fall out, often after a dose increase to 5 or 7.5 mg. Many people describe this moment as a shock, because the link in time to the medicine is not obvious.
- Months 4 to 6 (peak). The heaviest shedding phase, usually coinciding with the highest rate of weight loss. Importantly, the follicles are intact; there is no structural damage.
- Months 6 to 12 (recovery). As the weight loss slows, the shedding normalises. The first short, soft baby hairs become visible at the hairline and parting. Full cosmetic recovery takes 6 to 12 months after the weight has stabilised.
A note for people with a family history of hereditary hair loss: once the telogen effluvium has resolved, full density returns, provided there is no AGA in play. But if there is a genetic AGA that the effluvium has unmasked, a residual loss remains and continues to progress. In that case, a dermatological assessment after 6 to 9 months is strongly recommended.
Who is most at risk on Zepbound?
Not every Zepbound user loses hair. The risk depends on a few clear factors.
The single biggest factor. On 15 mg, around 57% of users in SURMOUNT-1 reach at least 20% weight loss. That puts more than half of those on the maximum dose in the high-risk group for a telogen effluvium.
According to the FDA label, women are affected at 7.1% versus 0.5% in men, a ratio of 14 to 1. A Canadian study (Sodhi et al. 2025) found a significantly raised hazard ratio of 2.08 for women, with no significant signal for men.
Anyone who speeds up the standard titration loses weight faster and so raises the risk. Losing more than 0.5 to 1.0 kg a week is considered a high-risk window.
Low ferritin, a zinc or vitamin D deficiency before starting treatment, and a family history of hereditary hair loss all raise the risk considerably. In one analysis, 91.4% of those affected had a previous history of hair loss.
What exactly is Zepbound?
Zepbound is a medicine from the manufacturer Eli Lilly, with the active ingredient tirzepatide. It is the first and so far only dual receptor agonist, activating both the GIP receptor (glucose-dependent insulinotropic polypeptide) and the GLP-1 receptor (glucagon-like peptide-1) at the same time. This double action explains why Zepbound produces greater weight loss than pure GLP-1 drugs such as semaglutide.
The FDA approved Zepbound on 8 November 2023 for chronic weight management, that is, for obesity (BMI of 30 or above) or excess weight (BMI of 27 or above) with at least one weight-related comorbidity. The crucial point for the hair question: it is exactly the same active ingredient as in Mounjaro, which is, however, licensed for type 2 diabetes. The standard titration is slow: starting at 2.5 mg a week, then a step up every four weeks (5, 7.5, 10, 12.5 mg) to the maximum dose of 15 mg from week 21.
The link with hereditary hair loss (AGA)
Many people carry a genetically determined predisposition to hereditary hair loss without realising it, because their hair is still dense enough. The telogen effluvium triggered by Zepbound can unmask this latent AGA. When follicles switch into the resting phase en masse, the genetically sensitive follicles that have already quietly miniaturised also shed their last hairs. The result: the person thinks Zepbound has caused fresh balding, when in fact the AGA was already present and is only now becoming visible.
The clinically important difference: with a pure telogen effluvium, full density returns. With unmasked AGA, a patterned residual loss remains and progresses. Where your hair loss sits on the scale can be gauged using the Norwood-Hamilton scale. A diffuse, even loss points towards an effluvium; recession at the temples or crown points more towards AGA.
One contrary finding is worth noting: in one documented case (Gordon et al., JAAD Case Reports 2024), tirzepatide actually improved hair growth in a man with AGA and pronounced insulin resistance, because the normalised insulin sensitivity had a favourable effect on local blood flow and DHT metabolism. The evidence is therefore not one-dimensional. For most patients with obesity on high doses, however, the effluvium risk from rapid weight loss clearly predominates.
Prevention: what you can do while losing weight
You can actively lower the risk without stopping treatment. The most effective levers lie in your diet and the pace of weight loss.
- Enough protein. The single most important measure. Aim for 1.2 to 1.6 g per kilogram of body weight a day, but at least 60 g a day, spread across several meals. With the sharply reduced appetite on Zepbound, it helps to deliberately prioritise protein-rich foods and, where needed, protein shakes.
- Check and correct micronutrients in a targeted way. Before and during treatment, have your ferritin (aim for above 40, ideally above 70 ng/mL), zinc, vitamin D and thyroid levels checked. Only supplement where a deficiency is confirmed.
- Ease off the pace. Stick to the standard titration schedule, at least four weeks at each dose step. Do not speed up the escalation. The clinical consensus is to limit weight loss to no more than 0.5 to 1.0 kg a week.
- Act when shedding begins. Pause the dose increase in agreement with your doctor, optimise your diet, and only titrate further once things have normalised.
The American Academy of Dermatology puts it this way: patients prone to hair loss should lose weight slowly while on weight-management medicines. The pace is the lever you hold most directly in your own hands.
Treatment and regrowth: what really helps
If the hair loss has already set in, there are several approaches with differing levels of evidence.
- Correct the deficiencies first. Without balanced iron, zinc and vitamin D levels, any further measure remains limited in effect. This is always the first step.
- Topical minoxidil. Used off-label in telogen effluvium, it stimulates the follicles to re-enter the growth phase early. A small open-label study (Ohyama et al. 2025) showed a marked improvement in hair density. More on this in our article on minoxidil for hair loss.
- Biotin: no benefit without a deficiency. In healthy people without a confirmed biotin deficiency, no efficacy has been shown. High-dose biotin also distorts laboratory tests such as troponin and thyroid hormones. Not recommended.
- PRP as an adjunct. Platelet-rich plasma therapy has solid evidence in female hair loss and AGA, and can be a sensible adjunct in persistent loss over six months.
In the vast majority of cases, the best treatment is patience plus optimising your diet. The telogen effluvium is self-limiting once the weight stabilises. A fuller explanation of diffuse hair loss can be found in our overview of telogen effluvium in general.
The Elithair approach: when is a hair transplant appropriate?
Here is the most important message for anyone losing hair on Zepbound: with a pure telogen effluvium, a hair transplant is not indicated. The follicles are structurally intact and the hair grows back on its own. A transplant would be medically unnecessary at this stage and technically not durable, because your own hair returns anyway.
A transplant only becomes relevant in a clearly defined scenario: when, after the effluvium has fully resolved, that is, at the earliest 12 months after the weight has stabilised, a lasting, patterned form of hair loss remains and medical AGA treatment is not enough. A hair transplant can then be the most permanent solution, because the transplanted hair comes from the DHT-resistant donor area and does not fall out again.
Many patients come to us in a panic because they have suddenly started losing hair on Zepbound. In most cases we can reassure them: it is a telogen effluvium caused by the rapid weight loss, and it grows back. We assess honestly whether any treatment is needed at all. We only recommend a transplant once a lasting, hereditary pattern remains after recovery.
Dr Balwi, Medical Director at Elithair
Zepbound compared with other GLP-1 medicines
The risk of hair loss differs markedly between the GLP-1 and GIP medicines, and the common thread is always the extent of weight loss. The table below places the most important products in context.
| Product | Active ingredient | Indication | Hair loss | Avg. weight loss |
|---|---|---|---|---|
| Zepbound | Tirzepatide | Obesity | approx. 5% vs. 1% placebo | −20.9% (15 mg) |
| Wegovy | Semaglutide | Obesity | approx. 3.3% vs. 1% placebo | −14.9% (2.4 mg) |
| Mounjaro | Tirzepatide | Type 2 diabetes | only in the label since Feb 2025 (post-marketing) | approx. −11% (15 mg) |
| Ozempic | Semaglutide | Type 2 diabetes | not in section 6.1 | approx. −5% (1 mg) |
Three findings stand out. First: Zepbound and Mounjaro contain the same active ingredient, tirzepatide, yet Zepbound has the markedly higher hair-loss signal, because in obesity it is used at higher doses and produces greater weight loss. With Mounjaro (diabetes), alopecia was only added retrospectively to the label as a post-marketing finding in February 2025. Second: within the obesity indication, Zepbound sits above Wegovy, the counterpart from the semaglutide family, which is consistent with its greater weight loss. Third: the diabetes drugs Ozempic and Mounjaro show the weakest signal, in line with the smallest weight loss. The indication is ultimately a proxy for the size of the weight loss.
When to see your GP or a dermatologist
Diffuse shedding from month 2 to 4 is normal and to be expected. Do not stop Zepbound on your own account because of it; instead, speak to your treating doctor. With the following signs, however, you should arrange a prompt assessment:
- Patchy, round hair loss (bald spots larger than 1 cm): suggests alopecia areata rather than telogen effluvium.
- Redness, severe itching, pain or scarring of the scalp: a possible sign of a scarring alopecia, in which hair loss can be irreversible. Early diagnosis is crucial.
- Marked hair loss in a man: since the label reports only a 0.5% incidence in men, any noticeable loss in a man particularly warrants assessment.
- No regrowth after 12 months or persistent loss over 6 months despite optimising your diet: suggests an accompanying, unmasked AGA.
Frequently asked questions about Zepbound and hair loss
Conclusion: does Zepbound cause hair loss?
Yes, Zepbound can trigger hair loss, and because it achieves the greatest weight loss of the entire drug class, the risk is highest here. But the key message is reassuring: the loss is almost always a temporary telogen effluvium, brought on by the rapid weight loss rather than by any poisoning of the hair roots. With enough protein, balanced micronutrients and a slow titration pace, the risk can be reduced considerably. In the vast majority of cases the hair grows back on its own 6 to 12 months after the weight has stabilised. A hair transplant only comes into the picture if a lasting, hereditary pattern remains after recovery. If you are unsure, the first step is worth taking and it is free: knowing what is really going on.
Sources
- Zepbound (tirzepatide) FDA Prescribing Information, section 6.1, Eli Lilly, 2024/2025. pi.lilly.com
- Jastreboff AM et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). NEJM 2022;387:205-216. NEJM
- Wadden TA et al. Tirzepatide for sustained weight reduction (SURMOUNT-3). Nat Med 2024. DOI
- Eli Lilly. SURMOUNT-5: Zepbound superior to Wegovy (head-to-head). zepbound.lilly.com
- Godfrey H et al. Alopecia associated with semaglutide and tirzepatide: FAERS disproportionality analysis. JEADV 2025. PMID: 38925559. PubMed
- Gupta AK et al. GLP-1 therapies and hair loss: A systematic review. Science Progress 2026. Sage Journals
- Vidal SI, Akiska YM et al. Increased incidence and risk of hair loss with GLP-1 receptor agonists. JAAD International 2026. PMC
- Rojas Lopez R et al. Alopecia as an Emerging Adverse Effect Associated With GLP-1 Receptor Agonists: A Scoping Review. Cureus 2025. PMC
- Gordon ER, Musleh S, Bordone LA. Treatment of insulin resistance with tirzepatide leading to improvement of hair loss. JAAD Case Reports 2024. PMID: 39135763. PMC
- Telogen Effluvium. StatPearls, NIH/NCBI, 2024. NCBI
- American Academy of Dermatology. How can GLP-1 drugs affect my skin, hair, and nails? 2026. aad.org
This article is for information only and is not a substitute for medical advice. If you have persistent hair loss, or before making any change to your medication, you should seek a professional diagnosis.

Dr. Imad Moustafa
Hair transplant specialist