
In short: finasteride for hair loss
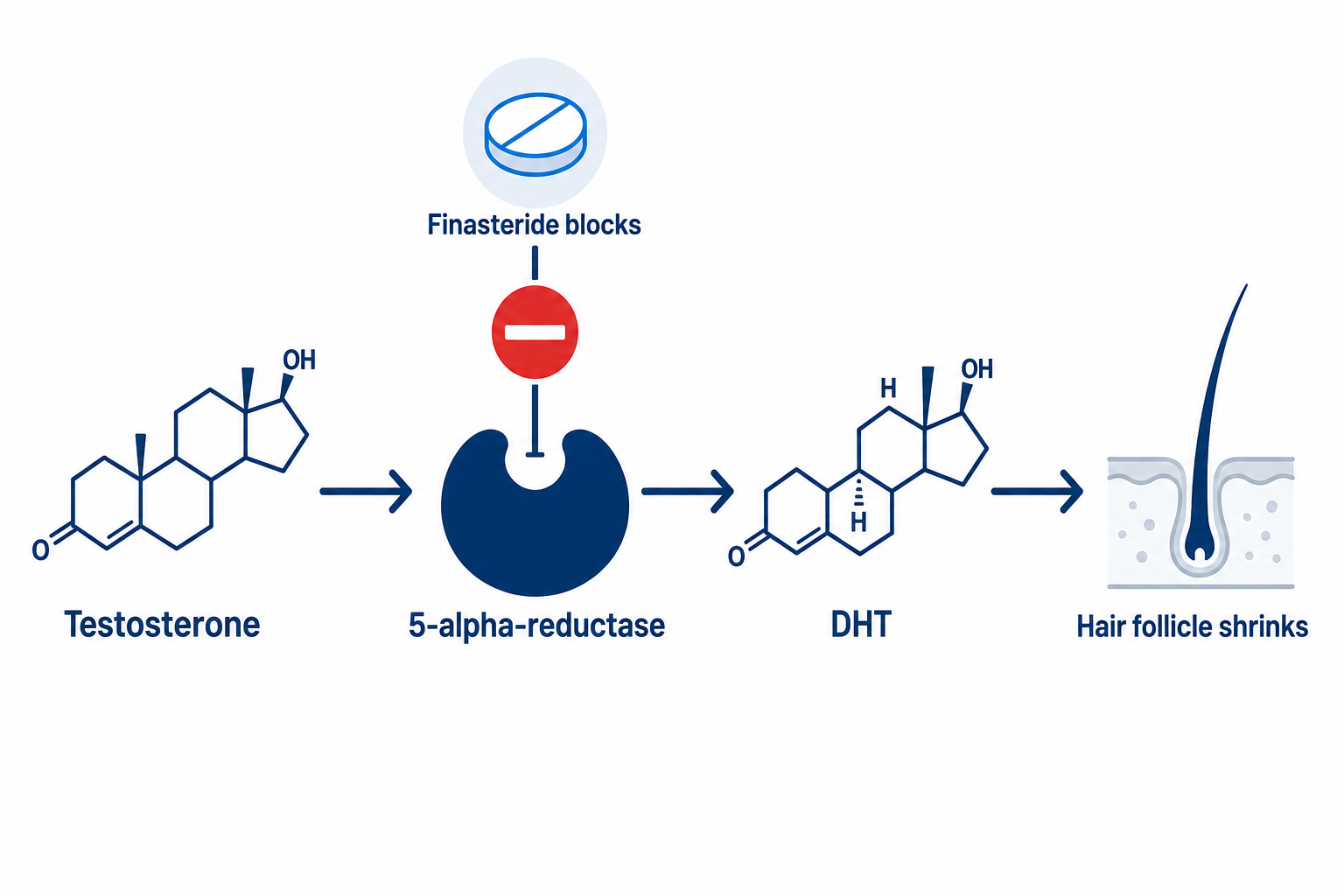
Finasteride is a prescription-only 5-alpha-reductase inhibitor that blocks the conversion of testosterone into dihydrotestosterone (DHT) and, in doing so, slows hereditary hair loss (androgenetic alopecia) in men. At a dose of 1 mg daily, hair loss stabilised in around 90 per cent of men over five years according to the registration trials, and some men saw visible regrowth. The effect lasts only for as long as the medicine is taken.
- ✓Drug class: 5-alpha-reductase inhibitor (type II), lowers serum DHT by about 71 per cent
- ✓Dose for hair loss: 1 mg daily (the 5 mg tablet is for the prostate)
- ✓prescription-only, not funded by the NHS as a cosmetic treatment
- ✓works only against androgenetic (hereditary) hair loss
- ✓reversible: after stopping, hair loss returns within 9 to 12 months
- ✓contraindicated for women of childbearing age (risk of malformations)
Finasteride is a medicine that carries real side effects. It is not something to self-medicate: it belongs in the hands of a doctor, including a proper discussion of the sexual and psychological side effects (as of 2026).
Summary
- What is finasteride and how does it work?
- How well does finasteride work against hair loss?
- How quickly does finasteride work? The timeline
- Taking finasteride correctly: the dosage
- How do I get a finasteride prescription?
- What does finasteride cost? Originator, generics and the NHS
- Topical finasteride: an alternative you apply to the scalp?
- Does finasteride distort the PSA value?
- What side effects does finasteride have?
- Post-finasteride syndrome and psychological effects: what is established?
- Stopping finasteride: what happens then?
- Can women take finasteride?
- Finasteride, minoxidil or dutasteride?
- Diffuse or genetic? When finasteride is the wrong approach
- Conclusion: finasteride at a glance (as of 2026)
- Frequently asked questions about finasteride
- Scientific sources
What is finasteride and how does it work?
Finasteride is a prescription-only medicine that slows hereditary hair loss in men by lowering DHT, the follicle-damaging hormone. Pharmacologically, finasteride is a 4-azasteroid and a selective inhibitor of type II 5-alpha-reductase. Its effect relies on blocking this enzyme, which converts testosterone into the considerably stronger dihydrotestosterone (DHT). According to the Propecia SmPC (Organon, as of August 2024), its selectivity for the type II isoform is more than 100 times higher than for type I.
Finasteride at a glance
| Feature | Detail |
|---|---|
| Drug class | 5-alpha-reductase inhibitor (type II) |
| Indication | androgenetic (hereditary) hair loss in men |
| Dose for hair loss | 1 mg daily, oral |
| Effect on DHT | lowers the serum DHT level by about 71 per cent |
| Onset of effect | first stabilisation after 3 to 6 months |
| Approved age group | men 18 to 41 years (registration trials) |
| Prescription and NHS | prescription-only, not funded by the NHS |
| Monthly cost (generic) | approx. £15 to £30 (as of 2026) |
| After stopping | hair loss returns within 9 to 12 months |
DHT is the central driver of androgenetic alopecia. Balding scalp skin contains raised levels of DHT, and the hormone shortens the growth phase (anagen) of genetically sensitive follicles. With each cycle the hairs become thinner and shorter, a process known as miniaturisation. Finasteride acts at precisely this root cause.
How strongly finasteride lowers DHT was shown by the dose-finding study by Roberts and colleagues (1999): at 1 mg daily, the serum DHT level fell by 71.4 per cent, and by 64.1 per cent on the scalp itself. The dose-response curve flattens out early: even 0.2 mg achieved most of the maximum possible reduction, and 5 mg added barely anything more.
That is precisely why 1 mg is the standard dose for hair loss. Finasteride works systemically, that is, throughout the whole body, in contrast to topical finasteride (more on that below) and to minoxidil, which acts purely locally and without any hormonal effect. To understand how the hair cycle works, with its anagen, catagen and telogen phases, see the article on the hair cycle.
How well does finasteride work against hair loss?
Finasteride for hair loss stops or slows hereditary hair loss in the majority of men, and some achieve visible regrowth. The evidence base is three randomised, placebo-controlled phase III trials involving 1,879 men aged 18 to 41 (Propecia SmPC, section 5.1). The key five-year figures:
- ✓Stabilisation: in 90 per cent (global photographic assessment) or 93 per cent (investigators), hair loss remained stable over five years.
- ✓Regrowth: an increase in hair growth was seen in 65 per cent (hair count), 48 per cent (expert panel) and 77 per cent (investigators).
- ✓Hair counts: after 2 years +88 hairs, after 5 years still +38 hairs per measured area, compared with -239 hairs on placebo after 5 years.
Kaufman and colleagues (2008) confirmed this independently: over five years, finasteride 1 mg reduced the risk of further visible hair loss compared with placebo by 93 per cent (95 per cent confidence interval 89 to 97, p less than 0.001). One caveat is that the number of men in the placebo group became small over the years. Even so, the trend in favour of finasteride is clear and has been shown repeatedly.
You have to stay honest about where it works. The effect is documented above all on the top of the scalp and in the crown area (vertex). For the bitemporal recession of the hairline, that is, the classic receding temples, and for end-stage hair loss, the SmPC states explicitly that no efficacy was demonstrated. Finasteride has no effect on follicles that are already completely lost: it does not make bald areas grow back.
That is why expectations have to match the stage. The Hamilton-Norwood scale helps to put the realistic benefit into perspective: the earlier the hair loss, the more can be preserved. With extensive baldness the medicine achieves next to nothing.
Realistic finasteride expectations by Norwood stage
| Norwood stage | Presentation | Realistic expectation |
|---|---|---|
| NW 2 to 3 | early receding temples, mild thinning | preservation very likely, some thickening on the top of the scalp |
| NW 3v to 4 | crown and top of the scalp affected | loss usually stabilisable, regrowth limited |
| NW 5 | larger bald areas | preserving the remaining density possible, bald areas remain |
| NW 6 to 7 | extensive baldness | little benefit, no effect on lost follicles |
A rough guide, not a prediction for the individual case. Assessing the stage and choosing the treatment belongs in the hands of a doctor.
How quickly does finasteride work? The timeline
How quickly finasteride works depends on the slow hair cycle: according to the SmPC, first signs of stabilisation are generally not expected until after 3 to 6 months of continuous use. The improvements in hair count were greatest after about 2 years and then slowly declined again, but remained clearly better than on placebo up to year 5.
| Time frame | What happens in the hair cycle | What you notice |
|---|---|---|
| Month 0 to 3 | DHT falls (by up to about 71 per cent), the environment around the follicle changes | usually no visible change yet, patience needed |
| Month 3 to 6 | the rate of shedding normalises | shedding noticeably eases (first stabilisation) |
| Month 6 to 12 | the anagen phase stabilises | visible thickening is possible on the top of the scalp |
| Month 12 to 24 | greatest effect around year 2, then a maintenance effect | plateau, effect only with continued use |
Individual courses vary. A lack of effect after 12 months should be discussed with a doctor.
A word on personal accounts and on what is known as initial shedding. Unlike with minoxidil, where an initial shedding phase is well documented, the SmPC does not list initial shedding as a separate side effect for finasteride. It is occasionally described in forums and personal reports, but it is not consistently documented and should not be equated with the better-documented minoxidil shedding.
Something else that shapes experiences with finasteride: those who start late or have a high Norwood stage less often experience visible regrowth and more often see preservation. That matches the trial data and is not a bad outcome, but simply the realistic expectation. Individual reports are no substitute for medical follow-up.
Taking finasteride correctly: the dosage
The finasteride dose for hair loss is 1 mg daily, with or without food, ideally at the same time of day. Oral bioavailability is around 80 per cent and is not affected by food (SmPC, section 4.2). Important: according to the SmPC, a higher dose is not more effective, because the reduction in DHT is already almost maximal at 1 mg.
The difference between 1 mg and 5 mg is therefore clear: the 5 mg tablet (such as Proscar) is licensed for benign prostatic enlargement, not for hair. Quartering it on your own or increasing the dose yourself is not a sensible route. In any case, the effect only exists with continuous use; a one-off course achieves nothing.
The subject of microdosing often comes up, meaning lower doses or taking it every other day to reduce side effects. In theory this can be inferred from the flat dose-response curve, but there is no controlled study comparing such a regimen with the daily 1 mg dose using hair-growth endpoints. It remains an off-label approach to be supervised by a doctor, not a standard therapy.
How do I get a finasteride prescription?
In the UK you can only obtain finasteride through a doctor or prescriber, because the active ingredient is prescription-only (SmPC, section 11). The first points of contact are your GP, a dermatologist or a urologist. The doctor makes the diagnosis, explains the benefits and risks, and prescribes finasteride if you are suitable.
Alongside this, reputable telemedicine providers offer an online prescription. After a medical questionnaire or a video consultation, a registered doctor issues the prescription, and the medicine comes via an online pharmacy. This route is legal, as long as a doctor is genuinely involved and you are informed about the risks, including the warnings on mood and suicidal thoughts flagged in the 2025 safety alert.
A warning about buying without a prescription: offers that promise finasteride without a prescription from dubious overseas pharmacies or online shops are risky. The active-ingredient content of such preparations is not guaranteed, and counterfeits and contamination do occur. Without medical advice, the important risk assessment (PSA value, psychiatric history, wish to have children) is also missing. Only buy finasteride with a prescription from a licensed pharmacy.
What does finasteride cost? Originator, generics and the NHS
As a generic, finasteride costs roughly between £15 and £30 per month as of 2026, depending on the provider and pack size; the originator product Propecia costs considerably more. Because finasteride for hair loss is not covered by the NHS, patients pay this amount themselves.
The active ingredient is identical in the originator and the generic. Since the patent expired there have been numerous 1 mg generics that contain the same active ingredient at the same dose and are usually many times cheaper than the originator Propecia. Medically, there is no difference in effect between the originator and an officially approved generic. Price is therefore the main argument for a generic.
The NHS does not fund finasteride for hair loss, even with a prescription. The reason: it is classed as a cosmetic (lifestyle) treatment rather than a medical necessity. For the prostate indication (5 mg) the funding position can be different, but that does not apply to hair-loss treatment.
Topical finasteride: an alternative you apply to the scalp?
Topical finasteride is applied directly to the scalp as a solution or spray and is intended to lower DHT locally, with less systemic exposure. In Europe it is no longer just a compounding grey area: with Finjuve (2.275 mg/ml spray, made by Almirall) there is a licensed finished medicine, applied once daily with 1 to 4 sprays in men aged 18 to 41.
Alongside this, individually compounded pharmacy formulations still exist, such as a 0.15 per cent finasteride solution, often combined with minoxidil. These have not gone through their own registration study. The rationale for topical finasteride is a smaller reduction in blood DHT and therefore potentially fewer systemic side effects. The long-term evidence, however, is thinner than for the oral preparation.
Important, with topical finasteride too: “only external, so harmless” is wrong. Applied finasteride can also transfer to others through skin contact (pillow, hands, towel). For pregnant women the same caution applies as with the tablet, because there is a risk of malformations in male foetuses. Let the application site dry, and avoid contact with pregnant women and children.
Does finasteride distort the PSA value?
Yes, finasteride lowers the PSA value, the most important blood marker in prostate-cancer screening. The SmPC states the practical rule verbatim: “A doubling of the PSA value should be considered in men taking Propecia before this test result is assessed.” Anyone taking finasteride must therefore inform every doctor treating them.
Specifically, the mean PSA in the studies of young men fell from 0.7 to 0.5 ng/ml after 12 months. The widespread rule of thumb of a halving comes from studies in older men on the 5 mg dose. It therefore makes sense to have a baseline PSA measured before starting treatment, so that later checks are interpreted correctly.
A common misunderstanding concerns the risk of prostate cancer. The often-cited PCPT study investigated 5 mg finasteride in men over 55 for cancer prevention, not the 1 mg hair-loss indication. There, the overall rate of prostate carcinomas fell by 24.1 per cent, while the proportion of higher-grade tumours was slightly higher. Transferring these data to the hair-loss treatment of young men would be misleading. To find out what a sensible blood test for hair loss looks like, see the separate article.
What side effects does finasteride have?
The most common finasteride side effects affect sexual function: reduced libido, erectile and ejaculation disorders. According to the SmPC, sexual side effects occurred in the first year in 3.8 per cent of finasteride users compared with 2.1 per cent on placebo. Over the following four years the frequency fell to 0.6 per cent. About 1 per cent stopped treatment for this reason in the first year.
- •Sexual side effects are mostly reversible and decrease over the course of treatment.
- •Depression is listed as “uncommon”, but in the randomised studies there was no difference from placebo.
- •Lumps, pain or discharge from the breast should be checked by a doctor promptly (rare reports of breast cancer in men).
| Side effect | Frequency (per the SmPC) | After stopping | Note |
|---|---|---|---|
| Reduced libido | uncommon | mostly reversible | most common sexual side effect |
| Erectile dysfunction | uncommon | mostly reversible | report to a doctor |
| Ejaculation disorders | uncommon | mostly reversible | incl. reduced ejaculate volume |
| Breast tenderness, gynaecomastia | not known | partly reversible | have lumps or discharge checked |
| Depression | uncommon | evidence unclear | no difference from placebo in studies, but take it seriously |
| Anxiety, suicidal thoughts | not known (spontaneous reports) | evidence unclear | 2025 safety alert, seek medical help immediately |
| Hypersensitivity (rash, urticaria, angioedema) | not known | after stopping | rare, have swelling checked by a doctor |
Frequency categories in the SmPC: uncommon = 1 to 10 per 1,000, “not known” = cannot be estimated from the available data (spontaneous reports). No substitute for a medical consultation.
Balance matters here: finasteride is neither harmless nor does it “guarantee impotence”. Most men tolerate it, a meaningful proportion do notice sexual side effects, which mostly resolve after stopping. The potential for interactions with other medicines is low according to the SmPC (metabolised via CYP3A4), but a medical discussion before starting remains a must.
Post-finasteride syndrome and psychological effects: what is established?
Post-finasteride syndrome (PFS) is the term for sexual, physical and psychological complaints that are said to persist after stopping finasteride. Whether finasteride causally triggers these complaints has not been conclusively established scientifically. The authorities take the reports seriously, but a straightforward proof of causation is still lacking to this day (as of 2026).
Regulation has tightened step by step. In 2012 the US authority FDA added notes on sexual dysfunction that can persist after stopping. In 2017 the EMA added a warning about mood changes including depression and, more rarely, suicidal thoughts, and assessed a causal link as “at least a plausible possibility”.
The most recent and most important piece of evidence is the safety alert issued in 2025 following an EU-wide review. That review identified 325 relevant cases of suicidal thoughts in the EudraVigilance database, dated 15 September 2025. In future, 1 mg packs will include a patient card. At the same time, the committee concluded that the benefit of finasteride continues to outweigh the risks.
Scientifically, PFS as a distinct condition is contested. A survey of Spanish dermatologists (2025) found that 98.1 per cent consider PFS to be more likely psychiatric or driven by a nocebo effect. Other, mechanistically oriented studies, by contrast, report measurable biological differences. Neither “PFS is proven” nor “PFS is pure imagination” is scientifically tenable.
What to do: in the case of depressed mood, a persistent low mood or suicidal thoughts while on finasteride, the SmPC and the safety alert state: stop the treatment and seek medical advice immediately. Do not simply carry on taking it, but do not stop on your own without medical supervision either. If you’re experiencing suicidal thoughts or a mental health crisis, help is available free of charge in the UK: call Samaritans on 116 123 (24/7) or text SHOUT to 85258. In a life-threatening emergency, call 999, or contact NHS 111 for urgent, non-emergency support.
Checklist: clarify with a doctor before starting finasteride
- ☐ Wish to have children and family planning (a semen analysis as a baseline if needed)
- ☐ History of depression or other psychiatric conditions
- ☐ Have a baseline PSA measured (finasteride lowers the PSA)
- ☐ Mention existing medicines and any liver disease
- ☐ Clarify expectations: preservation or regrowth, matching the Norwood stage
- ☐ Discuss alternatives (minoxidil, topical finasteride, hair transplant)
These points help in the conversation with your doctor, but are no substitute for medical advice.
Stopping finasteride: what happens then?
If you stop finasteride, DHT rises again and hereditary hair loss continues. According to the SmPC, the effects reverse within 6 months, and after 9 to 12 months the original, untreated state is reached again. The hair maintained by the therapy is lost over this period.
From this follows a central consequence for the decision: finasteride is a long-term therapy, not a one-off course. Anyone who wants to keep the result takes it continuously. Stopping should be done in consultation with a doctor, especially if the reason is side effects, so that alternatives can be considered together.
Can women take finasteride?
Finasteride is contraindicated for women of childbearing age. Because it inhibits the formation of DHT, if taken by a pregnant woman it can lead to malformations of the external genitalia of male foetuses (teratogenicity). Women who are pregnant or potentially pregnant must not even touch broken or crushed tablets, because of the possible absorption through the skin.
Important safety note (pregnancy): women who are pregnant or could be must not touch broken or crushed finasteride tablets. The active ingredient can be absorbed through the skin and cause malformations of the external genitalia in a male foetus. Intact film-coated tablets are safe under normal handling thanks to their coating. Keep the medicine out of the reach of pregnant women and children.
An often-overlooked figure also belongs to the topic of finasteride and women: in postmenopausal women with androgenetic alopecia treated for 12 months with finasteride 1 mg, no efficacy could be demonstrated according to the registration study. A Cochrane review rates the evidence in women overall as insufficient.
In women, moreover, diffuse hair loss often has other causes, such as iron deficiency or a thyroid disorder. Before any discussion of an active ingredient, therefore, comes the investigation of the cause. More on this in the article on hair loss in women, and on hormones in the article on hormones and hair.
Finasteride, minoxidil or dutasteride?
Finasteride, minoxidil and dutasteride act at different points: finasteride and dutasteride lower DHT (the cause), while minoxidil prolongs the growth phase locally, without any hormonal effect. The European S3 guideline on androgenetic alopecia (EDF, Kanti and colleagues 2018) lists topical minoxidil 5 per cent and oral finasteride 1 mg as therapies with a high level of evidence.
- •Combination: a meta-analysis of 7 randomised studies (n=396) found the combination of minoxidil and finasteride more effective than either monotherapy.
- •Dutasteride: inhibits both enzyme types and lowers DHT more strongly (about 90 to 93 per cent), but it is only licensed for the prostate. Its use for hair loss is off-label.
| Criterion | Finasteride | Minoxidil | Dutasteride | Hair transplant |
|---|---|---|---|---|
| Mechanism | inhibits 5-alpha-reductase, lowers DHT | prolongs the anagen phase, promotes blood flow | inhibits both 5-AR types (more strongly) | transplants DHT-resistant follicles |
| Use | oral, daily | topical (solution, foam) | oral | one-off procedure (FUE plus DHI) |
| Licensed for AGA (DE) | yes (men) | yes | off-label | established procedure |
| Works after stopping? | no (long-term therapy) | no (long-term therapy) | no | permanent |
| Systemic hormonal effect | yes (possible sexual side effects) | none (not a hormone) | yes (stronger) | none |
The comparison is factual, not a treatment recommendation. Which option or combination fits depends on the stage, the age and individual tolerability, and belongs to a medical discussion. Another, newer active ingredient is topical clascoterone, which blocks DHT locally at the follicle and is described in the article on clascoterone.
Diffuse or genetic? When finasteride is the wrong approach
Finasteride works exclusively against androgenetic, that is, hereditary hair loss, recognisable by the pattern with receding temples and a thinning top of the scalp or crown. Diffuse hair loss across the whole head due to iron deficiency, a thyroid disorder or other causes does not respond to finasteride. Here the cause should be investigated first, and often both forms occur at the same time.
That is why it is worth looking at the pattern. Diffuse thinning without a clear pattern points more towards telogen effluvium, for example due to an iron deficiency or a thyroid disorder. A look at the causes of hair loss and at the article on androgenetic alopecia helps with the assessment.

This is exactly where a hair analysis comes in. It clarifies which type is present before any decision about treatment is made. In advanced androgenetic alopecia with follicles that are already lost, finasteride can stabilise the existing hair, but cannot make bald areas grow back. For such areas, a hair transplant (FUE extraction plus DHI implantation) is the established, permanent option, because it transplants DHT-resistant hair from the back of the head.
Medicine and transplant are not mutually exclusive here. Accompanying medical maintenance is common practice to protect the non-transplanted, still DHT-sensitive native hair while the transplanted hair stays put. Elithair’s free hair analysis is a visual pattern analysis and helps to distinguish the genetic type from the diffuse type. It is no substitute for a medical blood test, which you should always have carried out if a deficiency is suspected.
A perspective from Elithair’s practice
Finasteride can slow hereditary hair loss, but it does not replace a diagnosis. In the consultation we first clarify which type of hair loss is present and whether the pattern fits androgenetic alopecia at all. Only then does a discussion about active ingredients, their benefit-risk profile or a transplant make sense. This order protects against false expectations.
Conclusion: finasteride at a glance (as of 2026)
Finasteride is the most effective oral standard therapy against hereditary hair loss in men, and in the registration trials it stabilised around 90 per cent of users over five years. It is a long-term therapy, works only on the androgenetic pattern and above all on the top of the scalp, and the effect ends when it is stopped.
At the same time, it is a medicine that carries real side effects, from sexual dysfunction to the warnings on mood and suicidal thoughts confirmed in the 2025 safety alert. The benefit and the risk can only be weighed up individually and with a doctor, especially where there is a wish to have children, a psychiatric history or problems with tolerability. The first step always remains a clean diagnosis.
Frequently asked questions about finasteride
How quickly does finasteride work?
According to the SmPC, first signs that hair loss is stabilising are generally not expected until after 3 to 6 months of continuous use. The greatest effect on hair count was reached in the studies after about 2 years. Patience is needed, because the hair cycle is slow.
What side effects does finasteride have?
The most common are sexual side effects such as reduced libido and erectile dysfunction, in the first year in 3.8 per cent compared with 2.1 per cent on placebo, mostly reversible. Also listed are depression and, as spontaneous reports, anxiety and suicidal thoughts (2025 safety alert). Have changes to the breast checked by a doctor.
What happens when you stop finasteride?
After stopping, DHT rises again. The effect reverses within 6 months according to the SmPC, and after 9 to 12 months the untreated starting state is reached. The hair maintained by the therapy is then lost, because finasteride is a long-term therapy.
Finasteride 1 mg or 5 mg?
Against hair loss, 1 mg daily is the licensed dose. The 5 mg tablet is intended for benign prostatic enlargement. A higher dose is not more effective for hair, because the reduction in DHT is already almost maximal at 1 mg. Do not change the dose on your own.
Can women take finasteride?
For women of childbearing age, finasteride is contraindicated, because it can cause malformations in a male foetus. In postmenopausal women, the registration study could not demonstrate any efficacy. Diffuse hair loss in women often has other causes such as iron deficiency or the thyroid, and should be investigated first.
Finasteride or minoxidil?
The two have different mechanisms: finasteride lowers DHT orally, minoxidil prolongs the growth phase locally without any hormonal effect. A meta-analysis of 7 studies found the combination more effective than either treatment alone. The European S3 guideline of 2018 lists both as therapies with a high level of evidence.
Is finasteride prescription-only, and does the NHS pay?
Finasteride is prescription-only in the UK. As a cosmetic (lifestyle) treatment it is not funded by the NHS, even with a prescription. The monthly cost for 1 mg generics is roughly £15 to £30 as of 2026.
Does finasteride cause permanent impotence?
No, that is not tenable as a blanket statement. According to the SmPC, erectile dysfunction is uncommon and mostly reversible after stopping. In rare post-marketing reports a persistence has been described, but a causal link has not been conclusively established. Always discuss any complaints with a doctor.
Does finasteride affect testosterone and muscle building?
Finasteride only blocks the conversion of testosterone into DHT, not the production of testosterone itself. The serum testosterone level usually stays stable or even rises slightly, mostly within the normal range. Finasteride has no performance-enhancing effect on muscle building, and a proven negative effect on the muscles is likewise not known.
Can I drink alcohol while taking finasteride?
The finasteride SmPC lists no direct interaction with alcohol, and according to the SmPC finasteride does not place an additional burden on the liver. Moderate alcohol consumption therefore does not, in principle, conflict with taking it. In the case of existing liver disease, however, the effect on metabolism has not been studied, and here a medical discussion is sensible.
Do I have to stop finasteride before or after a hair transplant?
Usually not. Finasteride is normally continued before and after a hair transplant, because it protects the non-transplanted, still DHT-sensitive native hair. This accompanying medical maintenance is common practice. Whether it is paused in an individual case is always decided by the treating doctor.
Scientific sources
- Propecia 1 mg film-coated tablets, prescribing information (Fachinformation), Organon Healthcare GmbH, as of August 2024. Organon (PDF)
- Roberts JL et al. (1999): Effects of finasteride on scalp skin and serum androgen levels in men with androgenetic alopecia. J Am Acad Dermatol. PubMed
- Kaufman KD et al. (2008): Long-term treatment with finasteride 1 mg decreases the likelihood of developing further visible hair loss. Eur J Dermatol. PubMed
- Kanti V, Messenger A, Dobos G et al. (2018): Evidence-based (S3) guideline for the treatment of androgenetic alopecia in women and in men. JEADV. PubMed
- EMA: Finasteride/dutasteride Article-31 referral, PRAC assessment report. EMA (PDF)
- Cochrane: Treatments for female pattern hair loss (CD007628). Cochrane
- Minoxidil-finasteride combined vs. monotherapy, systematic review and meta-analysis. PMC
This article is for general information and is no substitute for medical advice, diagnosis or prescription. Finasteride is prescription-only.

Dr. Imad Moustafa
Hair transplant specialist