
The hairline recedes at the temples, the forehead looks higher and the tell-tale M-shape starts to appear: a receding hairline is, for most men, the first visible sign of hereditary hair loss. This guide explains where it comes from, what actually slows it down, how to disguise it and when treatment makes sense. Updated 2026.
In short: what is a receding hairline?
A receding hairline is the wedge-shaped recession of the hairline at both temples (the classic “M” shape) and usually the first visible sign of androgenetic (hereditary) alopecia.
- The cause is overwhelmingly genetic and hormonal (DHT), not poor nutrition. Twin studies put the genetic component at around 80% (Nyholt et al. 2003).
- Yes, you can halt and slow it down (minoxidil, finasteride, evidence level 1 in the S3 guideline). The earlier you start, the more hair you keep. Receding temples growing back on their own without treatment essentially never happens.
- Only a hair transplant can reliably refill the receding corners themselves with your own hair.
- Preserving or restoring? If the goal is to preserve the hair you still have, medication helps. If corners that are already bald need filling back in, a transplant is the answer.
This guide is based on the European S3 guideline (Kanti et al. 2018) and is intended as general guidance. It does not replace a medical diagnosis. Prescription-only agents such as finasteride must only be used under medical supervision.
Summary
- What exactly is a receding hairline?
- When does it count as a receding hairline? Mature hairline vs. early hair loss
- Causes: why do you get a receding hairline?
- A receding hairline in men: Norwood stage, age and progression
- A receding hairline in women: rarer, but a warning sign
- Is a receding hairline a sign of going bald?
- Action plan: what to do when you spot a receding hairline
- How can you stop a receding hairline? Treatments compared
- Treating a receding hairline with a hair transplant
- Disguising a receding hairline: which haircuts help right away?
- When is it NOT a classic receding hairline?
- How long does it take to see something?
- Frequently asked questions about a receding hairline
- Sources
What exactly is a receding hairline?
A receding hairline is a wedge-shaped, triangular retreat of the hairline on both sides at the temples (medically, frontotemporal recession). It makes the forehead look higher and more angular, creating the typical “M” contour. It is part of the male pattern of androgenetic alopecia under the Hamilton-Norwood classification.
English has no single word for it: people simply speak of a receding hairline, receding temples or an M-shaped hairline. The German term “Geheimratsecken” (literally “privy councillor’s corners”) captures the old association neatly. From the 16th century, a “Geheimer Rat” was a high-ranking princely adviser, and these dignitaries were usually older men whose receding hairline came to be linked with age and standing (Gesellschaft für deutsche Sprache).
Why the temples first? The follicles at the forehead and temples carry considerably more androgen receptors and 5-alpha-reductase than those at the back of the head, where the protective enzyme aromatase predominates instead (Sawaya and Price, J Invest Dermatol 1997). It is precisely this distribution that later forms the basis of every hair transplant.
Not to be confused with a widow’s peak: this pointed, central V-shape at the hairline is an inherited, genetically fixed growth pattern present from birth (prevalence roughly 15 to 33%). It is not hair loss. A receding hairline, by contrast, develops over the course of life and progresses.
When does it count as a receding hairline? Mature hairline vs. early hair loss
We only speak of a truly receding hairline in the sense of hair loss once the recession progresses, deepens and the hair there begins to thin. A slight, symmetrical retreat of the hairline by about 1 to 2 cm compared with the childhood line, on the other hand, is a normal “mature hairline” and affects practically every man.
A commonly cited rule of thumb: a mature hairline is stable, even, sits about 1 to 1.5 cm above the juvenile line and shows no miniaturisation. Early androgenetic alopecia, by contrast, progresses year after year, can be asymmetrical, and the remaining hair becomes visibly finer and shorter.
That is why the trend over several months tells you more than a single snapshot. Comparing photos every few months shows far more reliably whether something is really changing than a scrutinising look in the mirror on any one day.

For young men: according to the European S3 guideline (Kanti et al. 2018), the first signs of androgenetic alopecia often appear as early as the teenage years. A stabilising maturation of the hairline at 17 to 20 is normal. Genuine, progressive recession this early points to an early-onset predisposition and is a good reason to have it checked medically now rather than later, because treatment started early preserves more hair.
Causes: why do you get a receding hairline?
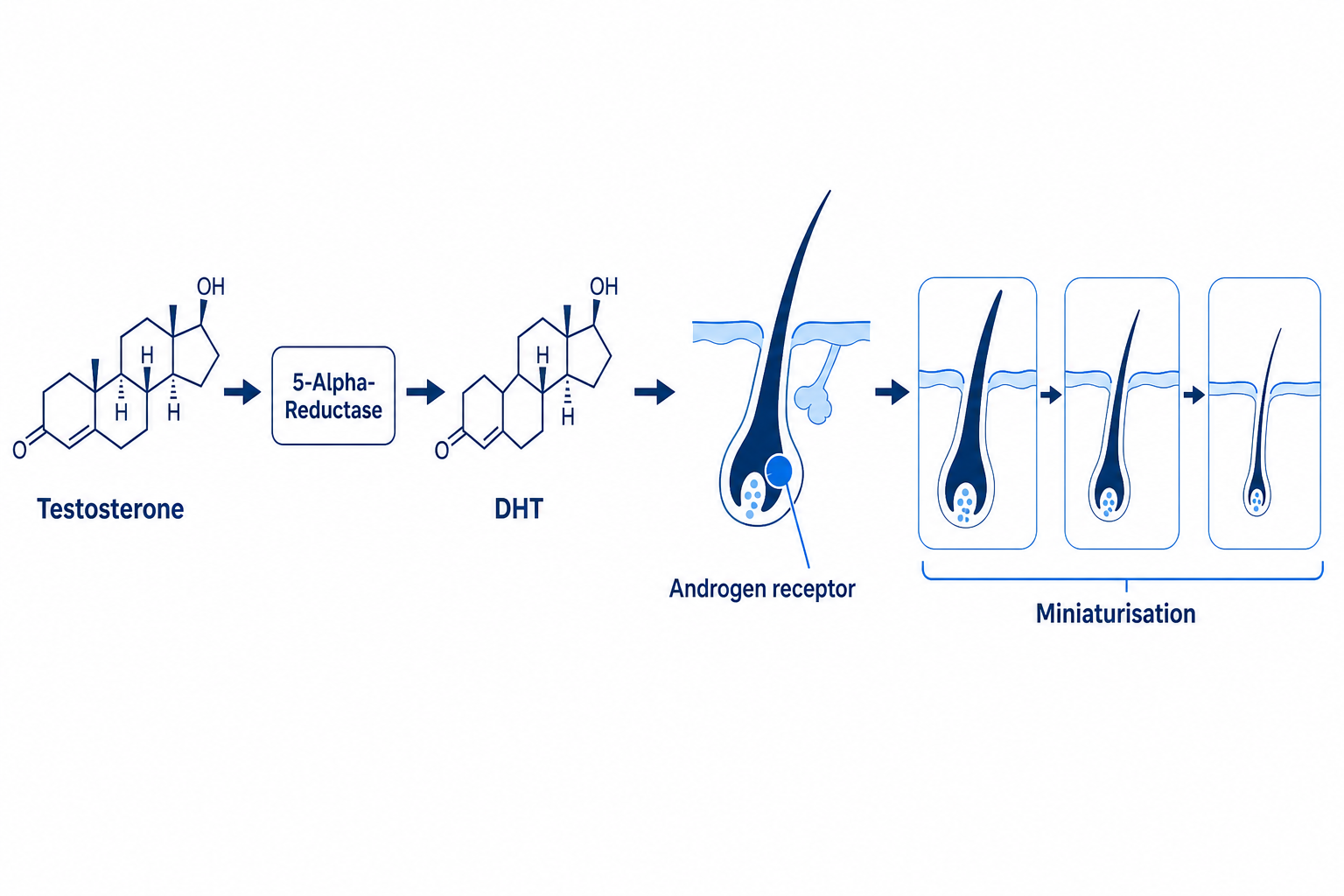
A receding hairline develops mainly through androgenetic alopecia. In this process, the hormone dihydrotestosterone (DHT) causes genetically sensitive hair follicles at the temples and crown to shrink over years (miniaturisation), until the hair there grows only as short vellus hair, or no longer at all.
The mechanism: testosterone is converted into DHT by the enzyme 5-alpha-reductase (above all type II). DHT binds to the androgen receptor of the sensitive follicles, shortens their growth phase and turns thick terminal hairs into thin vellus hairs. Over several hair cycles the hair becomes ever finer, until it stops coming through.
The predisposition is inherited polygenically and from both sides of the family. The widespread myth that hair loss comes “only from the mother” is false: the androgen receptor gene on the X chromosome explains less than half of the genetic variance, and another significant risk locus lies on chromosome 20p11 and is inherited independently of sex (Hillmer et al. 2008).
An important distinction: stress, iron deficiency or a thyroid disorder cause diffuse hair loss across the entire scalp (telogen effluvium), not wedge-shaped recession at the temples. If you are thinning more evenly, you will find more relevant answers in our guides to iron deficiency and hair loss, hair loss caused by the thyroid and vitamins against hair loss.
A receding hairline in men: Norwood stage, age and progression
In men, a receding hairline is the most common first symptom of hereditary hair loss and usually marks stage II to III on the Hamilton-Norwood classification. It begins at the temples and can later combine with a thinning crown (vertex).
Its frequency rises sharply with age: according to the European S3 guideline (Kanti et al. 2018), up to 80% of Caucasian men show signs of androgenetic alopecia by the age of 70. As a rough, frequently cited ISHRS guide: around 20% are affected in their 20s, about 30% in their 30s and roughly 40% in their 40s.
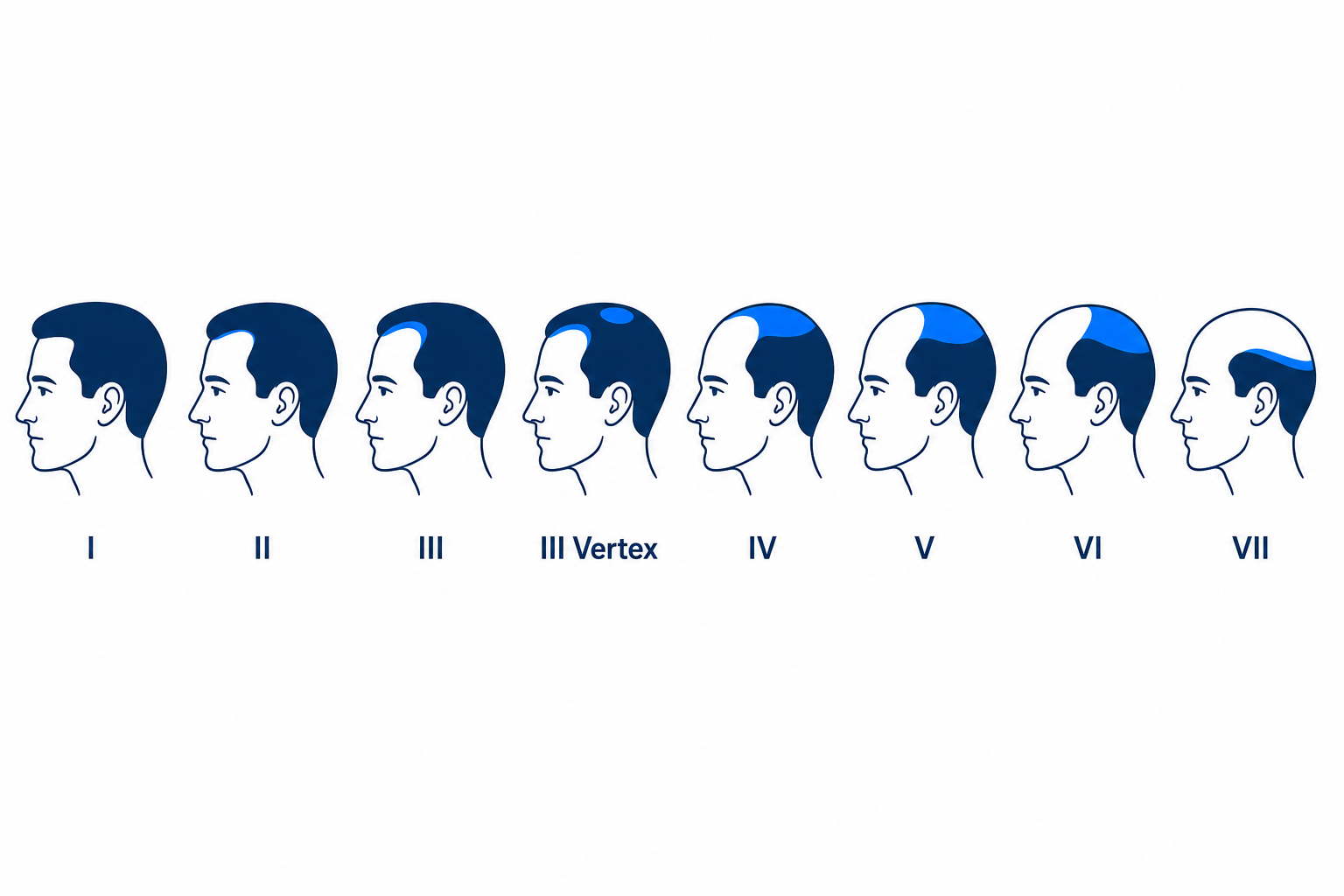
The Norwood scale helps you place your own stage roughly. The pace of progression is individual and strongly determined by genetics. An early onset already in puberty tends to go with a longer-running course, but this is not automatic.
| Norwood stage | Visible feature at the hairline | Meaning for a receding hairline |
|---|---|---|
| I | Straight, youthful hairline | No recession |
| II | Slight, symmetrical recession at the temples | Early receding hairline, often still a “mature hairline” |
| III | Deep, pronounced M-recession | Classic, treatment-relevant receding hairline |
| III Vertex / IV | Recession plus thinning crown / vertex | Progressing androgenetic alopecia |
| V to VII | Bald zones merging together | Advanced AGA, transplant requires careful donor-hair planning |
For guidance only, not a diagnosis. Certainty comes from a medical hair analysis. Classification after Hamilton (1951), modified by Norwood.
A receding hairline in women: rarer, but a warning sign
Women rarely develop a receding hairline in the classic M-shape. Female hereditary hair loss usually shows as diffuse thinning across the central parting with the front hairline preserved (Ludwig pattern), sometimes with the scalp showing through in a “Christmas tree” shape.
There is an enzymatic explanation: in women the androgen receptor content at the front is around 40% lower, while the protective aromatase activity is six times higher than in men (Sawaya and Price 1997). That is why the pattern is more diffuse and less sharply defined.
A genuinely, markedly receding hairline at the temples in a woman is therefore a warning sign that warrants dermatological assessment. It can point to frontal fibrosing alopecia (FFA), a scarring, irreversible form that mainly affects (post-)menopausal women and is accompanied by loss of the eyebrows in 80 to 95% of those affected (American Academy of Dermatology).
Hyperandrogenism (for example in PCOS) can also play a part. Reassuringly, though: according to the AE-PCOS Committee report (Carmina et al. 2019), most women with the fronto-central thinning pattern have normal androgen levels and no other symptoms. So isolated thinning is not automatically a hormonal alarm. Women should have the cause clarified before treating cosmetically. More on this in our guide to hair loss in women.
Is a receding hairline a sign of going bald?
A receding hairline does not inevitably mean full baldness later, but it is an early, reliable indicator of progressing androgenetic alopecia. How far the process goes is determined above all by genetic predisposition.
The course varies greatly from person to person. Some men stabilise for decades at Norwood stage II to III with a receding hairline alone, others progress to pronounced stages. An early onset and a strong family history on both sides count as prognostic pointers, though neither is deterministic.
The key point is this: the sooner the individual course is understood, the more precisely you can counteract it. Active agents work best while the follicles are still active. Which brings us to what actually to do.
A receding hairline is not just a matter of looks. In younger men especially, the glance in the mirror can gnaw at self-confidence, and the uncertainty about what is still to come often weighs more heavily than the hair loss itself. That worry is understandable and widespread. The best way out of the brooding is a clear, level-headed plan rather than frantically trying one product after another.
Action plan: what to do when you spot a receding hairline
If you notice a receding hairline, the best approach is four steps rather than randomly trying out products. This order saves time, money and disappointment. The links jump straight to the relevant section.
- Assess the stage. A rough self-assessment on the Norwood scale plus a photo comparison over several months. The trend matters more than the single day. → to the Norwood scale
- Confirm the cause medically. A dermatologist or hair analysis can clarify whether it really is genetic AGA or another form (diffuse, scarring, patchy). Don’t self-diagnose. → to the differential diagnosis
- Treat conservatively, as early as possible. Depending on the diagnosis, minoxidil and/or finasteride, under medical supervision. → to minoxidil and finasteride
- Consider a transplant only with a clear indication and after stabilisation; disguising is possible at any time in parallel. → to the hair transplant
How can you stop a receding hairline? Treatments compared
Stopping a receding hairline realistically means halting it and partly thickening it, not undoing it. With the right, medically supervised agents the course can be slowed; receding temples growing back on their own without treatment essentially never happens. The earlier you start, the more hair you keep.
Finasteride: the strongest evidence for halting it
Finasteride (oral, 1 mg/day) inhibits 5-alpha-reductase type II and lowers DHT durably by around 65%. In men it has the highest evidence level 1 in the European S3 guideline (Kanti et al. 2018), with a clear recommendation and long-term data over 60 months. The effect is judged after 6 months; in some men it only shows after 12 months.
Honest about the side effects: sexual dysfunction is possible, along with rare gynaecomastia and a depressive mood in those predisposed. Also discussed is post-finasteride syndrome (PFS), in which complaints are said to persist after stopping. The causality has not been conclusively established scientifically (S3 guideline). Finasteride is prescription-only, must be used under medical supervision and is contraindicated with active depression or existing sexual dysfunction. Women of childbearing age must not take it because of the risk of malformations.
Minoxidil: promotes growth, at the temples too
Minoxidil (topical, 2 to 5%) extends the growth phase of the hair and also has evidence level 1. The S3 guideline explicitly recommends it for the frontotemporal area as well, that is the temples, with 5% being more effective in men than 2%. The often-heard claim that minoxidil works less well at the hairline than at the crown is contested: the only direct comparative study found no clearly poorer response at the front after 8 weeks. You should therefore treat this point as an open discussion, not an established rule.
In the first few weeks, increased hair loss can occur (initial shedding), a sign of the effect setting in, not treatment failure. An important safety note that is often overlooked: minoxidil is highly toxic to cats. The ASPCA poison control centre recorded a 965% rise in reports between 2013 and 2024. Users with cats should wash towels and pillowcases and store any leftover product safely.
More on use and effect in the detailed guide minoxidil against hair loss.
Ketoconazole, dutasteride, microneedling and PRP
Ketoconazole shampoo (2%, e.g. Nizoral) has an anti-inflammatory effect on the scalp and is often named as part of the “Big 3”. The current S3 guideline gives it no recommendation, however, for lack of sufficient studies; it can be used as a supporting measure but is not a mainstay of treatment.
Dutasteride inhibits DHT even more strongly than finasteride, but in the UK and the EU it is not approved for hair loss. It only comes into question off-label and exclusively under medical supervision as a second-line option, when finasteride has failed over 12 months. It should not be promoted as a standard option.
Microneedling (dermaroller) shows no proven effect on its own, but combined with minoxidil it delivers solid additional benefits: a meta-analysis of 10 randomised studies with 466 patients (Archives of Dermatological Research 2025) found a large, significant advantage over minoxidil alone. PRP/mesotherapy can be considered as a supplement, but has evidence level 3 in the S3 guideline and, lacking a standardised protocol, no clear recommendation.
Home remedies for a receding hairline: the honest evidence check
No home remedy demonstrably reverses an advanced androgenetic recession, but the evidence base varies in strength. Rosemary oil achieved a result comparable to minoxidil after 6 months in a small randomised study (Panahi et al. 2015), but only against the weaker 2% concentration and in a single study. Caffeine has so far only stimulated hair follicles in cell-culture studies (Fischer et al. 2007); robust clinical data are lacking.
An important correction on onion juice: the much-cited study (Sharquie and Al-Obaidi 2002) was carried out on patients with patchy hair loss (alopecia areata), a completely different condition, not on androgenetic alopecia. So it cannot be applied to a receding hairline. Castor oil has no proven effect on follicle miniaturisation. Regard home remedies as care, not as a substitute for minoxidil or finasteride.
| Method | How it works | Evidence (S3 guideline 2018) | Limits / side effects |
|---|---|---|---|
| Finasteride (oral) | Lowers DHT | Level 1, recommended (men) | Prescription, sexual side effects possible, PFS discussed, contraindicated in women of childbearing age |
| Minoxidil (topical) | Extends the anagen phase | Level 1, recommended; 5% > 2% | Daily use, initial shedding, toxic to cats |
| Dutasteride (oral) | Stronger DHT inhibitor | Level 1, off-label / second-line only | Not approved for hair loss in the UK/EU, medical supervision only |
| Ketoconazole shampoo | Anti-inflammatory | Level 3, no recommendation | Supporting only, not a mainstay |
| Microneedling + minoxidil | Mechanical stimulation plus active agent | Meta-analysis 2025 significant | No effect solo, proven only in combination |
| PRP / mesotherapy | Growth factors from your own blood | Level 3, no recommendation | Series of sessions, cost, inconsistent data |
| Home remedies (rosemary oil/caffeine) | Care / mild stimulation | not robust for AGA | Does not reverse the recession |
| Hair transplant | Relocates more DHT-resistant native hair | Level 2, can be considered | Surgery, cost, only for pattern type with sufficient donor hair |
Evidence levels after the European S3 guideline (Kanti et al. 2018). No self-medication; prescription-only agents under medical supervision only.
Treating a receding hairline with a hair transplant
Moving on to a hair transplant is not about the medication having “failed”, but about the goal. Agents such as finasteride and minoxidil preserve the hair you have, as long as they are used continuously. What they cannot do is refill corners that are already bald. That is exactly where a transplant comes in as a permanent restoration.
Once the hairline has already receded markedly and is to be filled back in with dense, native hair, a hair transplant is the only treatment with a lasting result. It relocates far less androgen-sensitive hair roots from the back of the head into the bald corners. These keep their properties in the new location too, the so-called donor dominance principle (Kanti et al. 2018).
At Elithair the transplant is carried out as a DHI implantation with the CHOI pen, supported by the patented NEO FUE preparation. What decides a natural result is the hairline design: a deliberately irregular, age-appropriate line with single grafts at the very front edge instead of a hard “doll’s line”.

| Norwood stage | Rough graft requirement (corners / hairline) | Cost guide (Elithair fixed price, UK) |
|---|---|---|
| II (slight recession) | approx. 1,000 to 1,500 grafts | from £2,899 |
| III (pronounced M-recession) | approx. 1,500 to 3,000 grafts | approx. £2,899 to £2,999 |
| III + vertex | approx. 3,000 to 4,000 grafts (crown covered too) | approx. £2,999 to £3,199 |
Guide values, individual to the hair analysis. The final graft count and cost are set by the medical analysis. Details on the prices page and in the overview of the hair transplant.
A transplant, however, only makes sense with hereditary pattern hair loss, not with diffuse or scarring forms. Caution is especially warranted in young men in their early 20s: if the surrounding hair is not stabilised with medication and the loss continues to progress, an unnatural “island effect” can form around the dense transplant. The S3 guideline therefore stresses that the best long-term results are achieved with medically controlled or stabilised AGA.
The first step is therefore not surgery, but the diagnosis. A free hair analysis determines your Norwood stage, distinguishes genetic from diffuse hair loss and tells you honestly whether and when a transplant makes sense for you. Our overview shows real results: before and after with a receding hairline.
A note from Elithair’s practice
A receding hairline is one of the most rewarding starting points for a hair transplant, because the donor zone at the back of the head is genetically far less androgen-sensitive. Two things decide the result: a natural, irregular hairline design and the accompanying medical control of the rest of the hair loss. Without this combination, a procedure remains risky in young patients who are still progressing.
Disguising a receding hairline: which haircuts help right away?
You disguise a receding hairline best with short, textured haircuts that deliberately break up the hairline rather than emphasising it. This is the purely cosmetic level alongside medical treatment: it does not tackle the cause, but works immediately and can be done in parallel at any time. Long hair combed back and a slick centre parting, by contrast, make the recession stand out visually.
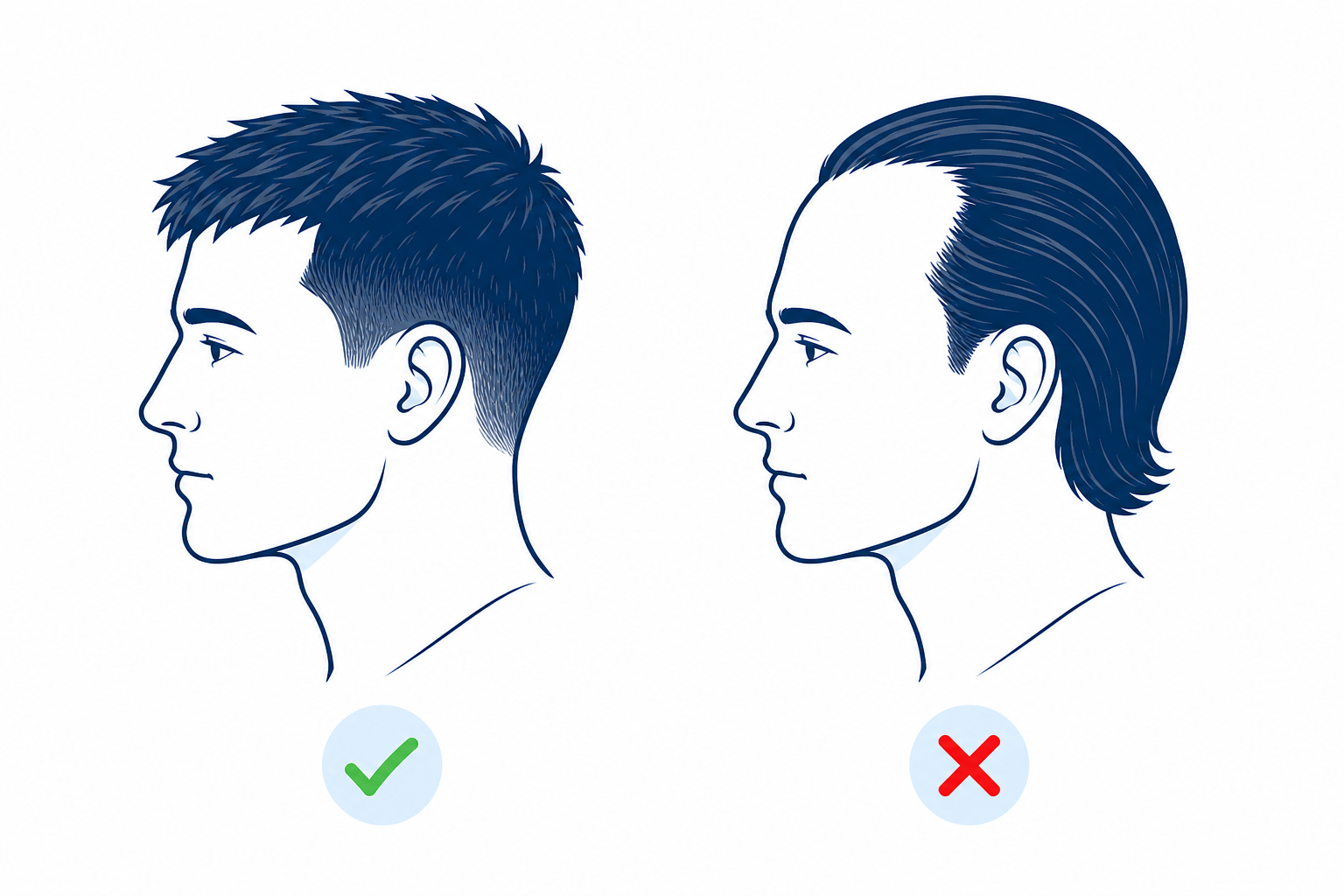
The basic rule: short sides combined with textured top hair swept forward (French crop, Caesar cut, buzz cut, possibly with a beard), a deliberately short, defined rather than frayed line, and matte rather than shiny products. Avoid the classic comb-over and long top hair, which only makes the gaps visible.
| Disguises a receding hairline | Emphasises it (avoid) |
|---|---|
| Short textured cuts (French crop, Caesar) | Long hair gelled back |
| Fringe swept forward | Slick centre parting |
| Defined, deliberately short hairline | “Frayed”, thin edge |
| Matte products, beard to lead the eye | Shiny gel that reveals gaps |
| Hair fibres, hairline concealer | Comb-over |
Face shape plays a part too. In brief: angular faces carry a buzz cut or skin fade with confidence, oval ones a textured French crop, round faces benefit from more height on top and longer faces from shorter fringes that visually shorten the forehead.
| Face shape | Recommended cut |
|---|---|
| Angular / strong | Buzz cut / skin fade |
| Oval | French crop with texture on top |
| Round | More height and volume on top, short sides |
| Long | Shorter fringe, visually shorten the forehead |
And the question that troubles many: should you shave your hair really short? A very short shave or a skin fade makes the recession almost disappear visually, because there is no longer any contrast between the dense and thinning areas. That is a legitimate, immediately available and confident choice, not giving up. For women, a side parting instead of a centre parting and colour-matched root powder help.
When is it NOT a classic receding hairline?
Not every receding hairline is hereditary. A mature hairline, diffuse (telogen) hair loss, traction alopecia and scarring forms can look similar to androgenetic recession, but need different assessment and treatment. This distinction is the reason the diagnosis comes before any treatment.
With telogen effluvium, the hair falls out evenly across the entire scalp, not in a wedge shape at the temples. Common triggers are iron deficiency, thyroid disorders or severe stress. Traction alopecia develops through constant pulling (tight braids, buns, extensions) and is reversible in the early stage once the strain ends (American Academy of Dermatology). Alopecia areata shows round, sharply defined bald patches and is autoimmune in origin.
Red flags: when you should see a doctor
- Very rapid, sudden hair loss
- Round, patchy bald spots instead of wedge-shaped recession
- Itching, redness, scaling or a shiny, scarred scalp
- A woman with markedly receding temples (not a normal parting pattern)
- Loss of the eyebrows (especially in women, a pointer to FFA)
- Hair loss together with fatigue, cycle disturbances or weight change
In these cases: see a dermatologist or endocrinologist, no self-treatment.
To clarify the cause, a look at the overall situation and, in part, blood values make sense. How a blood test helps is covered in the guide blood test for hair loss, and an overview is offered by causes of hair loss.
How long does it take to see something?
Patience is essential, because the hair cycle takes several months. With medication you see a reliable stabilisation after about 6 months at the earliest, and the final result of a transplant after 9 to 12 months at the earliest. Anyone who gives up after 4 weeks is judging too soon. More on the growth phases in the guide hair cycle.
| Method | First reaction | Result you can judge |
|---|---|---|
| Minoxidil | Initial shedding in the first few weeks | after approx. 6 months |
| Finasteride | Stabilisation from month 3 to 6 | 6 to 12 months |
| PRP | over a series of sessions | several months |
| Hair transplant | Shock loss week 2 to 6, new hair from month 3 to 4 | full result month 12, maximum density month 18 |
Timings after the S3 guideline (Kanti et al. 2018) and Elithair’s healing course. Varies individually.
Frequently asked questions about a receding hairline
What exactly is a receding hairline?
A receding hairline is the wedge-shaped recession of the hairline at both temples (the typical M-shape) and usually the first visible sign of androgenetic (hereditary) alopecia.
When is it a receding hairline rather than a normal hairline?
When the recession goes beyond the normal, stabilising “mature hairline” (about 1 to 2 cm), progresses and the hair there becomes thinner. A stable, even maturation, by contrast, is normal.
A receding hairline at 20, is that normal?
A slight maturation of the hairline in late puberty is normal. Genuine, progressive recession this early points to early-onset AGA (first signs often already in the teenage years, Kanti et al. 2018) and is a good reason for early assessment, not a reason to panic.
Receding hairline or widow’s peak, what is the difference?
A widow’s peak is an inherited, genetically fixed V-shape at the hairline that is present from birth and is not hair loss. A receding hairline develops over the course of life and progresses.
Can you stop or reverse a receding hairline, does the hair grow back?
Halting and slowing it, yes, with medically supervised agents (finasteride, minoxidil, evidence level 1). Spontaneous regrowth of corners that are already bald, without treatment, essentially never happens. Only a transplant can reliably refill lost hair there.
Does minoxidil help with a receding hairline?
Yes, minoxidil is recommended in the S3 guideline for the frontotemporal area (the temples) too. Whether it actually works less well at the hairline than at the crown is scientifically contested and not consistently proven.
Does microneedling or a dermaroller help?
On its own there is no proven effect. Combined with minoxidil, though, newer meta-analyses (Archives of Dermatological Research 2025) show a significant improvement over minoxidil alone.
Do women get a receding hairline too?
Rarely in the classic M-shape. More common is diffuse thinning at the parting (Ludwig pattern). A genuine temple recession in a woman is a warning sign and should be assessed by a dermatologist.
Which haircut disguises a receding hairline best?
Short, textured cuts with top hair swept forward (French crop, Caesar cut). You should avoid long hair combed back, a centre parting and a comb-over.
Should I shave my hair really short because of a receding hairline?
A very short shave or a skin fade is a legitimate, immediately available and confident option, because the contrast between the dense and thinning areas disappears. That is not giving up.
Is a receding hairline a sign of going bald?
Not inevitably, but an early indicator of progressing androgenetic alopecia. How far it goes is determined above all by genetic predisposition.
At what age do you get a receding hairline?
First signs often already in the teenage years. Prevalence rises with age to up to 80% of men at 70 (Kanti et al. 2018).
What does a hair transplant for a receding hairline cost?
Depending on the Norwood stage, the requirement is roughly 1,000 to 4,000 grafts, and the Elithair fixed-price range is about £2,899 to £3,199. The exact figure is only set by the hair analysis.
Do home remedies like rosemary oil or caffeine shampoo help?
Rosemary oil showed a result comparable to minoxidil 2% in a small study, caffeine so far only in cell-culture studies. Neither demonstrably reverses an advanced recession.
Sources
- Kanti V, Messenger A, Dobos G et al. (2018): Evidence-based (S3) guideline for the treatment of androgenetic alopecia in women and in men. J Eur Acad Dermatol Venereol 32:11-22. Link
- Nyholt DR et al. (2003): Genetic basis of male pattern baldness. J Invest Dermatol 121(6):1561-1564. Link
- Sawaya ME, Price VH (1997): Different levels of 5alpha-reductase type I and II, aromatase, and androgen receptor in hair follicles of women and men with androgenetic alopecia. J Invest Dermatol. Link
- Panahi Y et al. (2015): Rosemary oil vs minoxidil 2% for the treatment of androgenetic alopecia. Skinmed 13(1):15-21. Link
- Carmina E et al. (2019): Female Pattern Hair Loss and Androgen Excess (AE-PCOS Committee). J Clin Endocrinol Metab 104(7):2875-2891. Link
- Systematic review and meta-analysis of microneedling + minoxidil (2025), Archives of Dermatological Research. Link
- American Academy of Dermatology (AAD): Frontal fibrosing alopecia. Link
- ASPCA: Minoxidil and Pets, What You Need to Know. Link
- Gesellschaft für deutsche Sprache (GfdS): on the origin of the word Geheimrat. Link
This article is for information and does not replace medical advice, diagnosis or treatment. Prescription-only agents and surgical procedures require an individual medical assessment. Updated 2026.

Dr. Imad Moustafa
Hair transplant specialist