
In brief: what is trichotillomania?
Trichotillomania is a recognised mental health condition in which people repeatedly give in to a strong urge to pull out their own hair, usually from the scalp, eyebrows or eyelashes. It belongs to the body-focused repetitive behaviours (BFRBs) and is not a lack of willpower. Clear improvement is possible with behavioural therapy.
- Classification: ICD-11 code 6B25.0, placed within the obsessive-compulsive spectrum in the DSM-5.
- Lifetime prevalence of roughly 0.5 to 2 per cent depending on the study, with a suspected high number of undiagnosed cases.
- Best treatment: behavioural therapy, above all habit reversal training. A hair transplant does not treat the disorder.
- As long as the follicles are intact, the hair usually grows back once the pulling stops.
Note: this article is for information only and is not a substitute for medical or psychotherapeutic advice, diagnosis or treatment.
Summary
- What is trichotillomania?
- Trichotillomania: causes and psychological triggers
- Who is affected? Frequency, age and body areas
- Is trichotillomania a compulsion, an addiction or self-harm?
- Trichotillomania test: how do I recognise the disorder?
- Trichotillomania or alopecia areata? The important difference
- Treating trichotillomania: what really helps
- What helps in everyday life? Immediate coping strategies
- Does the hair grow back after pulling?
- Can trichotillomania cause permanent hair loss? And when a hair analysis makes sense
- Trichotillomania in children: what parents should know
- Concealing bald patches in everyday life
- Outlook: do people grow out of trichotillomania?
- Trichophagia and Rapunzel syndrome
- Frequently asked questions about trichotillomania
- Conclusion
- Sources
What is trichotillomania?
Trichotillomania, also known as pathological hair pulling, is a mental health condition within the spectrum of body-focused repetitive behaviours (BFRBs). The WHO lists it in the ICD-11 under code 6B25.0, related to skin-picking disorder. People pull out their own hair repeatedly, even though they do not want to.
In the DSM-5, trichotillomania sits in the chapter “Obsessive-Compulsive and Related Disorders”, alongside obsessive-compulsive disorder and skin-picking disorder. One important sign of how the understanding has moved on: in the older ICD-10 it was still classed as a “disorder of impulse control”. The new placement in the ICD-11 reflects today’s understanding of it as a distinct BFRB.
Specialists distinguish two patterns. With automatic pulling, people only notice it afterwards, for example while reading or watching television. With focused pulling it is a deliberate act, often triggered by feeling a hair perceived as “wrong”, with tension beforehand and relief afterwards (Grant & Chamberlain, 2016).
One thing to be clear about: trichotillomania is not a bad habit or a character flaw. What sets the disorder apart from a mere habit is a key DSM-5 criterion: repeated attempts to stop fail despite the distress it causes. The exact neurobiological mechanisms remain “largely unexplained”, according to the German medical journal Deutsches Ärzteblatt.
Trichotillomania: causes and psychological triggers
The causes of trichotillomania are multifactorial. There is no single cause, but an interplay of genetic predisposition, altered processing of stimuli in the brain, and psychological triggers such as stress, tension, anxiety, boredom or sadness. In the short term, pulling relieves tension, which reinforces the behaviour.
This is precisely where the central psychological cause of hair pulling lies. According to Deutsches Ärzteblatt, pulling is usually triggered not by a specific external event but by generally heightened inner tension. The pulling brings brief relief. This reward cements the behaviour and turns it into a learned self-soothing pattern.
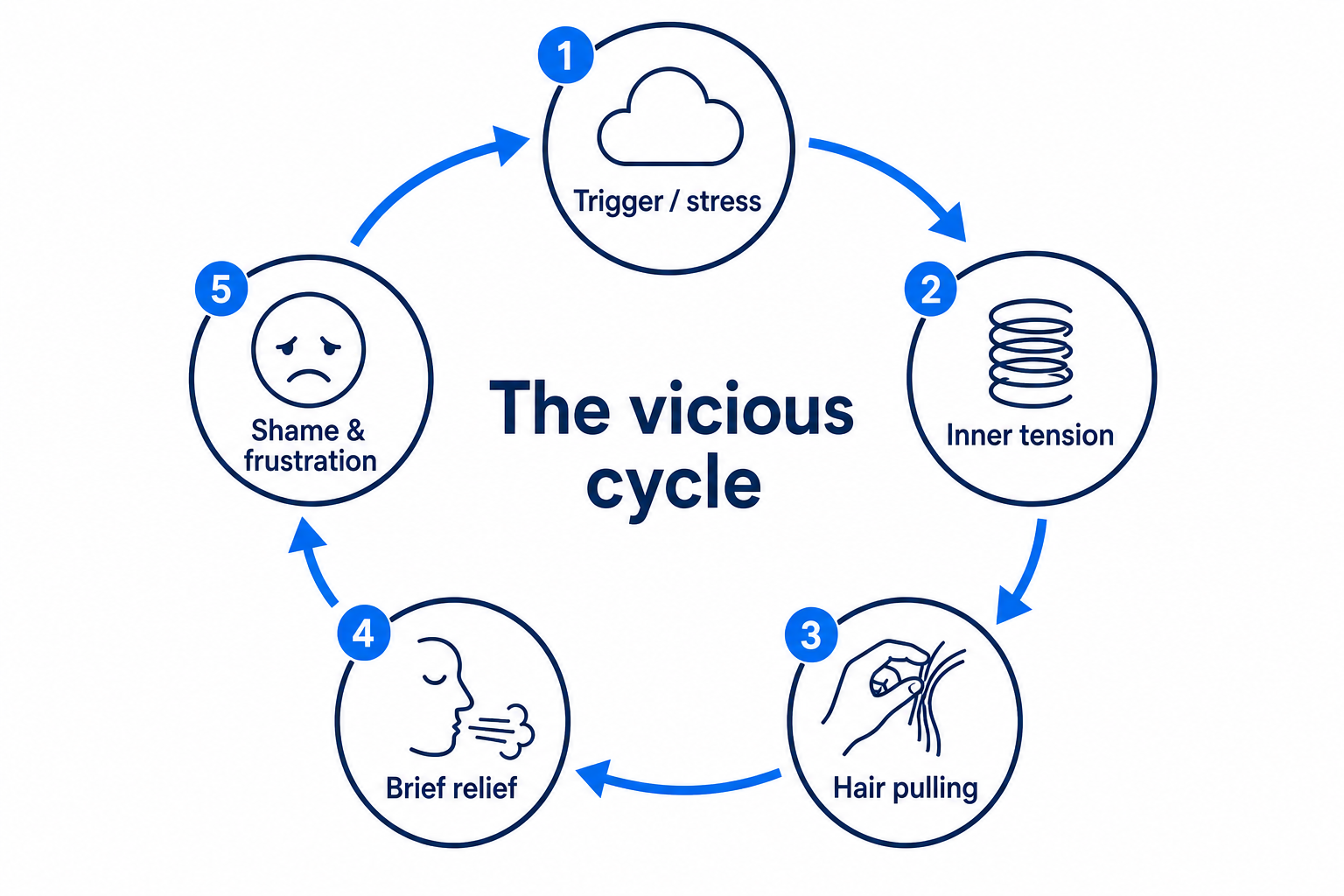
This cycle explains why simply “pulling yourself together” rarely works: a trigger or inner tension leads to the urge, the urge to pulling, pulling to short-term relief, and often afterwards to shame or frustration, which raises the tension again. This reinforcement pattern is the basis of the effective behavioural therapies (see Treatment).
Some people report distressing experiences such as bullying, violence or abuse as a possible contributing trigger. But this does not apply to everyone: specialists stress that many people start with no identifiable trigger at all, for instance out of boredom. Trichotillomania is therefore not an inevitable consequence of trauma, and no one has to squeeze themselves into a category that does not fit.
Other mental health difficulties often occur alongside it. The review by Grant and Chamberlain reports major depression in 39 to 65 per cent, anxiety disorders in 27 to 32 per cent and obsessive-compulsive disorder in 13 to 27 per cent of those affected. Importantly, trichotillomania usually begins before these accompanying conditions, so it is a distinct disorder and not a consequence of them. More on the causes of hair loss in our overview.
Who is affected? Frequency, age and body areas
Trichotillomania typically begins in early puberty. Grant and Chamberlain describe the age of onset across studies and cultures as “remarkably consistent” at around 10 to 13 years. According to the patient information resource DEXIMED, around two-thirds of those affected develop the disorder during puberty.
The sex distribution shows a clear pattern: in childhood, boys and girls are affected about equally, while in adulthood women predominate at a ratio of roughly 4:1 (Grant & Chamberlain, 2016). This difference may be partly due to under-reporting in men. For more on female hair loss in general, see hair loss in women.
Hair is pulled most often from the scalp, followed by the eyebrows and eyelashes, and less often from the beard and body hair. The ICD-11 description explicitly names the scalp, eyebrows and eyelashes as typical areas. These sites are a symptom of the disorder, not a case for cosmetic correction: treatment always starts with the behaviour.
A special case is hair pulling in young children under about five years old. It often occurs as self-soothing when falling asleep, similar to thumb-sucking, and is usually harmless and temporary. Even so, any bald patch in a child should be checked by a doctor (more on this in the section for parents).
Is trichotillomania a compulsion, an addiction or self-harm?
Trichotillomania is not a classic addiction and not deliberate self-harm, but a distinct body-focused repetitive behaviour within the wider obsessive-compulsive spectrum. This classification comes from the DSM-5 and is more than a question of wording: it determines the right therapy.
The difference from obsessive-compulsive disorder (OCD): with classic compulsions, the ritual is usually preceded by anxiety-laden, intrusive thoughts that are meant to be neutralised. In trichotillomania, this element is absent in many people; the tension-relief pattern is what stands out. A co-occurring obsessive-compulsive disorder is present in a minority, however.
The difference from non-suicidal self-injury: there, the injury is usually the deliberate aim. In trichotillomania, hair loss is a consequence of regulating tension, not its purpose. People generally do not want to harm themselves, but to reduce inner tension. There are parallels with addiction in the reinforcement mechanism, but it is not a substance or behavioural addiction in the narrow sense.
Trichotillomania test: how do I recognise the disorder?
A genuine trichotillomania test in the sense of a diagnosis exists only with a specialist doctor or psychotherapist. A professional makes the diagnosis based on the five DSM-5 criteria in conversation. In clinical practice and research, the Massachusetts General Hospital (MGH) Hairpulling Scale by Keuthen et al. (1995) serves as the standard tool for tracking progress, not for self-diagnosis.
Important: this is not a diagnostic test, but a first orientation. It is not a substitute for medical or psychotherapeutic assessment. If several points apply to you, speak to a doctor or psychotherapist.
Orientation self-check (based on the DSM-5 criteria)
- I repeatedly pull out my own hair, so that hair is visibly missing.
- I have tried several times, without success, to stop or cut down.
- The pulling distresses me significantly or affects my daily life, work or social contacts.
- The hair loss cannot be explained by a skin condition.
- It cannot be better explained by another mental health condition.
Additional everyday signs
- The pulling happens mainly during stress, tension or boredom.
- There is a ritual with the hair (feeling for it, twirling it, examining the root).
- I hide bald patches or avoid certain situations because of them.
Clinical warning signs support the assessment but prove nothing on their own: irregularly shaped bald areas with hairs of different lengths and broken-off stubble, often on the side of the head that is easy to reach for the dominant hand, without the smooth, freshly shaved-looking skin of alopecia areata.
Trichotillomania or alopecia areata? The important difference
Trichotillomania and alopecia areata both cause bald patches, but they are fundamentally different. Trichotillomania is psychologically driven, mechanical pulling. Alopecia areata is an autoimmune condition in which T-cells attack the hair follicle. A dermatologist can tell them apart reliably, among other things through trichoscopy.
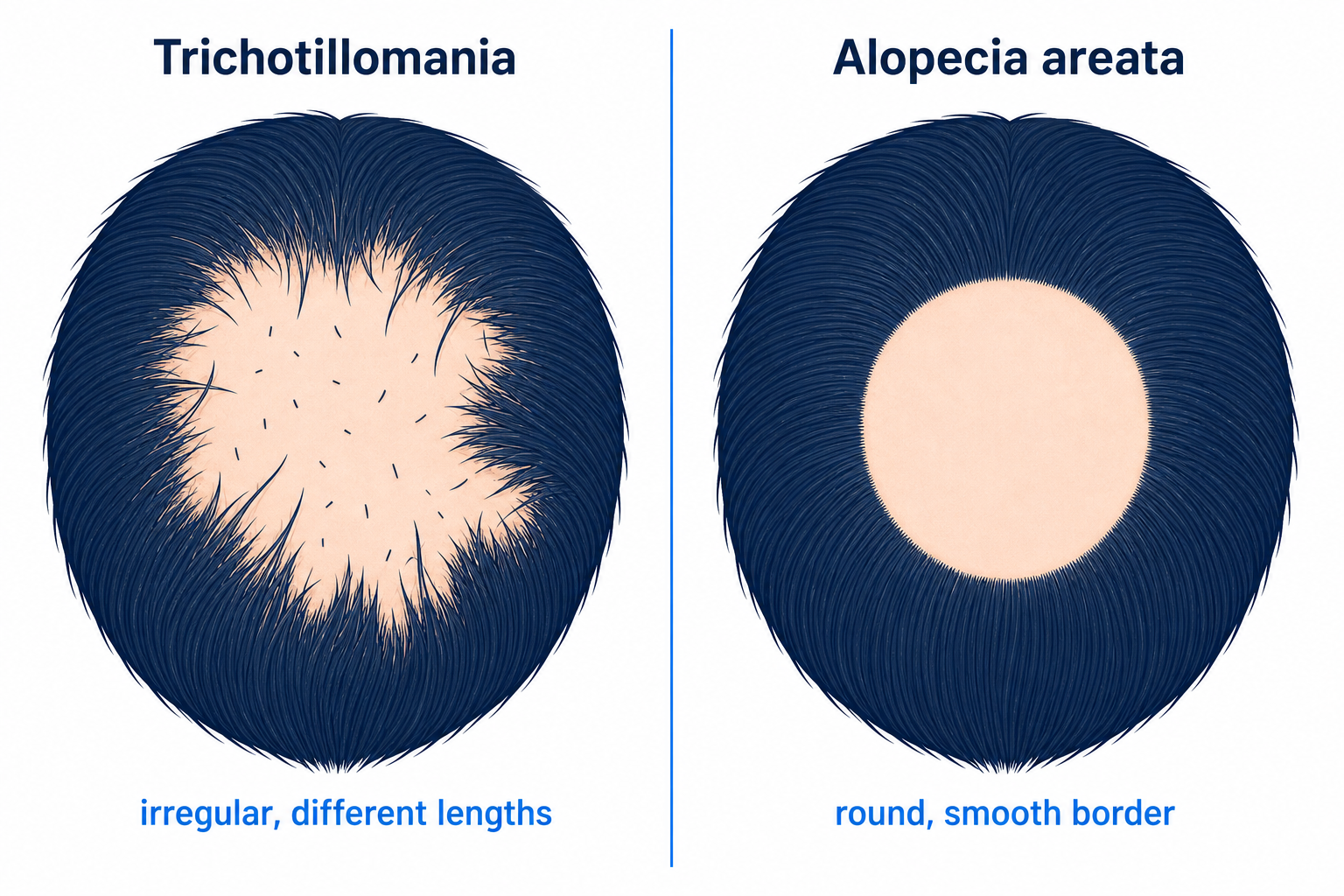
The distribution pattern is the first clue: alopecia areata produces round, sharply defined, smooth patches. In trichotillomania the areas are irregularly bordered and contain hairs of different lengths. Under the trichoscope the picture becomes clear, as the following overview shows.
| Feature | Trichotillomania | Alopecia areata |
|---|---|---|
| Cause | psychologically driven, mechanical pulling | autoimmune condition (T-cell attack on the follicle) |
| Pattern/shape | irregular, often angular border, on the easy-to-reach side | round, sharply defined, smooth bald patches |
| Hairs in the area | hairs of different lengths, broken-off stubble | usually completely bald and smooth |
| Skin | unremarkable, possibly slight irritation | smooth, “as if freshly shaved” |
| Trichoscopy | V-sign, flame hairs, hook hairs, coiled hairs | exclamation-mark hairs, yellow and black dots |
| Treatment | behavioural therapy (habit reversal training) | dermatological (including corticosteroids, JAK inhibitors) |
The trichoscopy signs are well documented: according to a systematic review of diagnostic accuracy, hook hairs (100 per cent specificity), the V-sign (99 per cent) and coiled hairs (99.6 per cent) are highly specific for trichotillomania. According to Rakowska et al. (2014), the V-sign occurs in 58 per cent of trichotillomania cases but in only 8 per cent of alopecia areata. More on this in the article alopecia areata.
Treating trichotillomania: what really helps
The most effective treatment for trichotillomania is a specific form of behavioural therapy, habit reversal training (HRT), often complemented by the ComB model. Medication is a second choice, and none is licensed specifically for trichotillomania.

Psychotherapy: the first choice
Habit reversal training is the evidence-based first-line therapy. It combines self-monitoring (awareness training), practising a competing response, and stimulus control, typically over 4 to 22 sessions. An older meta-analysis placed HRT, with an effect size of Cohen’s d of around −1.14, clearly above drug treatment.
Just how clear the difference can be is shown by a controlled Dutch comparison study (n=43) cited by Deutsches Ärzteblatt: six sessions of behavioural therapy led to a 64 per cent reduction in symptoms, the antidepressant fluoxetine to just 9 per cent, and the waiting-list control group to 20 per cent. The sample was small, but the direction was unambiguous in favour of behavioural therapy.
The ComB model (Comprehensive Behavioural Model) by Charles Mansueto extends HRT with an individual analysis of triggers across five domains (sensory, cognitive, affective, motor and environmental). It is regarded as a useful addition in more complex or chronic cases. To be honest: relapses are part of the course of the condition, more on that below.
Medication: second choice, medically supervised only
Among medications, N-acetylcysteine (NAC) is discussed most often. In a double-blind, placebo-controlled study by Grant, Odlaug and Kim (2009) in the journal Archives of General Psychiatry (n=50 adults), 56 per cent of the NAC group improved significantly, compared with 16 per cent on placebo. However, NAC is not licensed specifically for trichotillomania, and it should only be taken under medical supervision.
Particularly important for parents: a paediatric study found no difference between NAC and placebo in children and adolescents (response rate 25 versus 21 per cent). For young people, behavioural therapy is therefore clearly the priority. SSRIs such as fluoxetine are considered to have weak evidence and are usually only used for accompanying conditions such as depression, as a case-by-case medical decision.
| Approach | What happens | Who for | Note / evidence |
|---|---|---|---|
| Habit reversal training | awareness, competing response, stimulus control | first choice, all age groups | best evidence base |
| ComB model / extended CBT | trigger analysis across five domains | complex, chronic cases | complements HRT |
| N-acetylcysteine (NAC) | amino acid, medically prescribed only | mainly adults, as an add-on | limited evidence, not licensed, no better than placebo in children |
| SSRIs / other medication | mostly for accompanying conditions | case-by-case medical decision | evidence weak and inconsistent |
| Self-help / support groups | everyday strategies, sharing, relief | complementary for everyone | not a substitute for therapy |
Self-help and where to turn
Alongside therapy, support organisations can help with getting your bearings. In the UK, charities such as OCD Action offer guidance, and internationally the TLC Foundation for BFRBs (bfrb.org, founded in 1991) provides a directory of self-help resources and professionals. The following overview shows what to look for in your search.
Finding the right help: a short guide
- Search terms: “behavioural therapy”, “habit reversal training”, “trichotillomania / skin-picking experience”, “body-focused repetitive behaviour”.
- Appointment: in England you can refer yourself to NHS Talking Therapies without a GP referral; elsewhere in the UK, ask your GP about talking therapies.
- Organisations: UK charities such as OCD Action, and internationally the TLC Foundation for BFRBs.
- Children and young people: child and adolescent psychotherapy with experience in BFRBs.
What helps in everyday life? Immediate coping strategies
Small behavioural barriers and greater mindfulness can ease the urge to pull in the moment. This immediate help is not a substitute for therapy, but it supports it. The following points are derived from habit reversal training and match the simple, practical tips from the UK’s NHS.

Everyday quick-help card
- Keep a trigger diary: note down when and where the urge appears.
- Use a competing response: clench your fist, squeeze a spiky ball or stress ball, use a fidget toy.
- Use physical barriers: gloves, plasters on your fingertips, a hat or cap, short fingernails.
- Defuse triggers: put tweezers, mirrors and plucking tools out of sight.
- Keep your hands busy: in risky situations such as watching TV or reading, deliberately pick something up.
These strategies support you, but they are not a substitute for professional treatment when distress persists.
A trigger diary reveals the patterns you would otherwise miss. Over a few days, note down in which situation the urge appears, what feeling came before it and what helped. The following examples show what such entries can look like.
| Situation (where / when) | Feeling beforehand | Response / what helped |
|---|---|---|
| In the evening in front of the TV | tension, boredom | squeezed a spiky ball |
| At my desk while working | concentration, inner restlessness | covered fingertips with plasters |
| In bed before falling asleep | ruminating, tension | hands under the duvet, short breathing exercise |
| In the bathroom in front of the mirror | searching for “irregular” hairs | dimmed the light, left the room |
| In the car, in a traffic jam | frustration, impatience | gripped the steering wheel firmly, chewed gum |
Does the hair grow back after pulling?
In most cases, the hair grows back after trichotillomania. As long as the follicles are intact, they resume their activity once the pulling stops for good. The first fine hairs usually become visible over a few months. Only with very long, repeated pulling can individual follicles be permanently damaged.
The reason lies in the natural hair cycle: once the pulling strain is removed, the follicles that were initially in the resting phase (telogen) re-enter the growth phase (anagen). The following timeline is a rough guide based on general hair-growth physiology, not a study figure specific to trichotillomania.
| Time frame | What happens | Condition |
|---|---|---|
| Month 1–2 | pulling stopped, irritated follicles recover | follicles intact |
| Month 3–4 | follicles enter the growth phase (anagen) | reversible |
| Month 4–6 | first new hairs visible, often fine or coiled | reversible |
| from month 6+ | increasing density, texture normalises | reversible |
| Special case | no or incomplete regrowth where there is scarring | long-standing chronic course |
The decisive factor is duration: occasional or short-term pulling usually only leads to temporary thinning. Pulling repeatedly at the same spot over years, on the other hand, can permanently damage the follicles through repeated mechanical strain. Be cautious with predictions: there is no fixed regrowth timeline proven for trichotillomania.
Scalp care during the recovery phase
During the recovery phase, the scalp above all needs gentle treatment after pulling. Clean the affected areas gently and without vigorous rubbing, and avoid harsh styling products, heat and tight hairstyles that pull on the hair. Any further mechanical strain can delay the follicles’ recovery. If redness, flaking, crusting or signs of inflammation appear, this should be checked by a dermatologist.
Can trichotillomania cause permanent hair loss? And when a hair analysis makes sense
Permanent hair loss from trichotillomania is rare. Short-term pulling usually does not damage the follicles for good. Only years of repeated pulling can act as a form of traction alopecia and, via chronic inflammation, lead to scarring in which functioning follicle tissue is replaced by scar tissue. There is no reliable frequency figure for this risk; it is based on clinical experience and case reports.
This leads to a clear order of priorities. The first and most important step is always the psychotherapeutic treatment of the disorder. A hair transplant is contraindicated while pulling is active, because transplanted hair would be pulled out just the same and the underlying condition would remain untreated. It is not a solution for trichotillomania.
Only after stable remission, that is, when the pulling has stopped for good, and only for remaining areas that are no longer regrowing, does the question of restoration arise at all. A hair analysis in the form of a visual pattern analysis via trichoscope can then assess whether the follicles are reversibly irritated or permanently damaged. It is not a substitute for a medical diagnosis, but it helps to distinguish reversible from scarred.
A note from Elithair’s practice
“Under the trichoscope, in a hair analysis we can often tell whether bald patches are caused by mechanical pulling or by alopecia areata. As long as pulling is active, we clearly advise against a hair transplant. The first step is always psychotherapeutic treatment. Restoration can only be considered at the earliest after stable remission, and only for areas that have finished scarring.”
Elithair medical team
If, after successful treatment, the question turns to remaining, scarred areas, Elithair works with the extraction of individual grafts (FUE) and DHI implantation. This concerns only the cosmetic result after completed behavioural therapy, never the disorder itself. A free hair analysis can, in this case, clarify whether the areas are reversible or scarred.
Trichotillomania in children: what parents should know
In young children, hair pulling is often a temporary phase within self-soothing, frequently alongside thumb-sucking or nail-biting. According to the TLC Foundation, the outlook in young children is largely favourable, and the pulling often stops on its own. Even so, the rule stands: any bald patch in a child should always be checked by a paediatrician.
This assessment rules out physical causes such as a skin condition or alopecia areata, or sources of stress such as teething. Do not rely on a blanket “they’ll grow out of it”. In the school and teenage years, where the disorder often begins at 10 to 13 years old, an assessment by a child and adolescent psychotherapist is advisable.
As for how parents should behave: stay calm, offer reassurance, and do not punish or shame. On heredity: a familial clustering is documented, and a genetic contribution is assumed. But a predisposition is not automatic; most children of affected parents do not develop trichotillomania. Also keep an eye on whether your child puts pulled-out hair in their mouth (see trichophagia).
| Better not to say or do | What really helps |
|---|---|
| “Just stop doing it” | show understanding, take it seriously as a disorder |
| reproaches, shaming, constantly catching them out | encourage and support professional help |
| slapping hands away or policing them | distract together mindfully, acknowledge successes |
Concealing bald patches in everyday life
Until the hair grows back, bald areas can be discreetly covered up. Concealing is expressly allowed and is not giving up: it lowers the level of distress while the actual treatment is under way. The only important thing is that concealing does not replace the therapy.
Practical options include hair fibres (keratin fibre powder for thin areas), adapted hairstyles with a repositioned parting, scarves, hats or bandanas, and, for larger areas, a hairpiece. For eyelash or eyebrow loss, subtle cosmetic stopgap solutions can help. The NHS likewise names hats and bandanas as practical self-help.
One note: hairstyles that constantly pull on the hair, such as tight braids or extensions, place extra strain on the already stressed areas and should be avoided during the recovery phase. The aim is to spare the follicles any further mechanical strain.
Outlook: do people grow out of trichotillomania?
In young children, the pulling often disappears on its own. If trichotillomania begins in puberty or adulthood, however, it usually runs a chronic and fluctuating course, with better and worse phases. According to DEXIMED, it becomes considerably more persistent once it lasts longer than six months, and rarely resolves on its own without treatment.
With behavioural therapy, clear improvement is realistic, as the 64 per cent reduction in symptoms in the Dutch study shows. At the same time, honesty matters: according to a systematic review, 50 to 67 per cent of initial responders experience a relapse over the long term. A relapse during stressful periods is therefore common and is not a personal failing, but part of the typical course.
Trichophagia and Rapunzel syndrome
Some people eat the pulled-out hair, which is known as trichophagia. Swallowed hair can compact in the stomach into a hairball (trichobezoar). If this extends into the small intestine, it is called Rapunzel syndrome, a very rare but serious medical emergency.
Rapunzel syndrome is exceptional: up to 2019, according to a case review, around 120 cases had been described in the world literature, of which about 90 per cent were women and around 80 per cent were under 30 years old. Warning signs are abdominal pain, nausea, a feeling of fullness, unexplained weight loss or a palpable abdominal mass. If these occur in someone with known trichophagia, this should be assessed by a doctor without delay.
Frequently asked questions about trichotillomania
Which doctor treats trichotillomania?
The right professionals are psychotherapists and psychiatrists with experience in obsessive-compulsive and related disorders, and for children, child and adolescent psychotherapy. A dermatologist can help to distinguish trichotillomania from other forms of hair loss.
Does the NHS cover treatment for trichotillomania?
Yes. Behavioural therapy such as CBT is available on the NHS. In England you can refer yourself to NHS Talking Therapies without seeing your GP first; in other parts of the UK, ask your GP about talking therapies.
How long does it take for the hair to grow back?
As a rough guide based on the hair cycle: the first fine hairs often become visible over 3 to 6 months after stopping, while full density takes longer. There is no fixed, study-backed timeline specifically for trichotillomania.
Can you stop trichotillomania on your own?
Partly. Everyday strategies such as a trigger diary, competing responses and physical barriers can ease the urge. When distress persists, however, they are not a substitute for professional treatment.
How do I deal with trichotillomania at the hairdresser or with people around me?
You do not have to explain yourself to anyone. Many people give a brief heads-up to a hairdresser they trust, so that bald patches are handled sensitively. With those close to you, it helps to point out matter-of-factly that this is a recognised disorder, not a bad habit.
Is trichotillomania curable?
The word “curable” is not quite the right fit. But trichotillomania is very treatable, and clear improvement up to remission is realistic. Relapses during stressful periods are common and not a failure, but part of the typical, fluctuating course.
Conclusion
Trichotillomania is a treatable mental health condition, not a lack of willpower. Behavioural therapy, above all habit reversal training, is demonstrably more effective than medication on its own. The most important step is therefore to seek professional psychotherapeutic help, rather than blaming yourself.
As for the hair: in most cases it grows back once the pulling stops, because the follicles are intact. A hair transplant is not a substitute for treatment and is contraindicated while pulling is active. As of 2026, the clear message stands: treat the disorder first, then think about any remaining areas.
Sources
- Grant JE, Chamberlain SR (2016). Trichotillomania. American Journal of Psychiatry.
- Grant JE, Odlaug BL, Kim SW (2009). N-Acetylcysteine in the treatment of trichotillomania. Archives of General Psychiatry.
- Rakowska A et al. (2014). New trichoscopy findings in trichotillomania. Acta Dermato-Venereologica.
- Diagnostic Accuracy of Trichoscopy in Trichotillomania. Acta Dermato-Venereologica.
- Habit Reversal Therapy in Obsessive Compulsive Related Disorders (Systematic Review). PMC / Frontiers.
- WHO ICD-11: 6B25.0 Trichotillomania. ICD-11 reference.
- German Society for Obsessive-Compulsive Disorders: Trichotillomania. zwaenge.de.
- Deutsches Ärzteblatt: Trichotillomania, a puzzling mental health condition. aerzteblatt.de.
- NHS: Trichotillomania. nhs.uk.
This article is for information only and is not a substitute for medical or psychotherapeutic advice, diagnosis or treatment. If you suspect trichotillomania, consult a doctor or psychotherapist. Last updated: 2026.

Dr. Imad Moustafa
Hair transplant specialist