
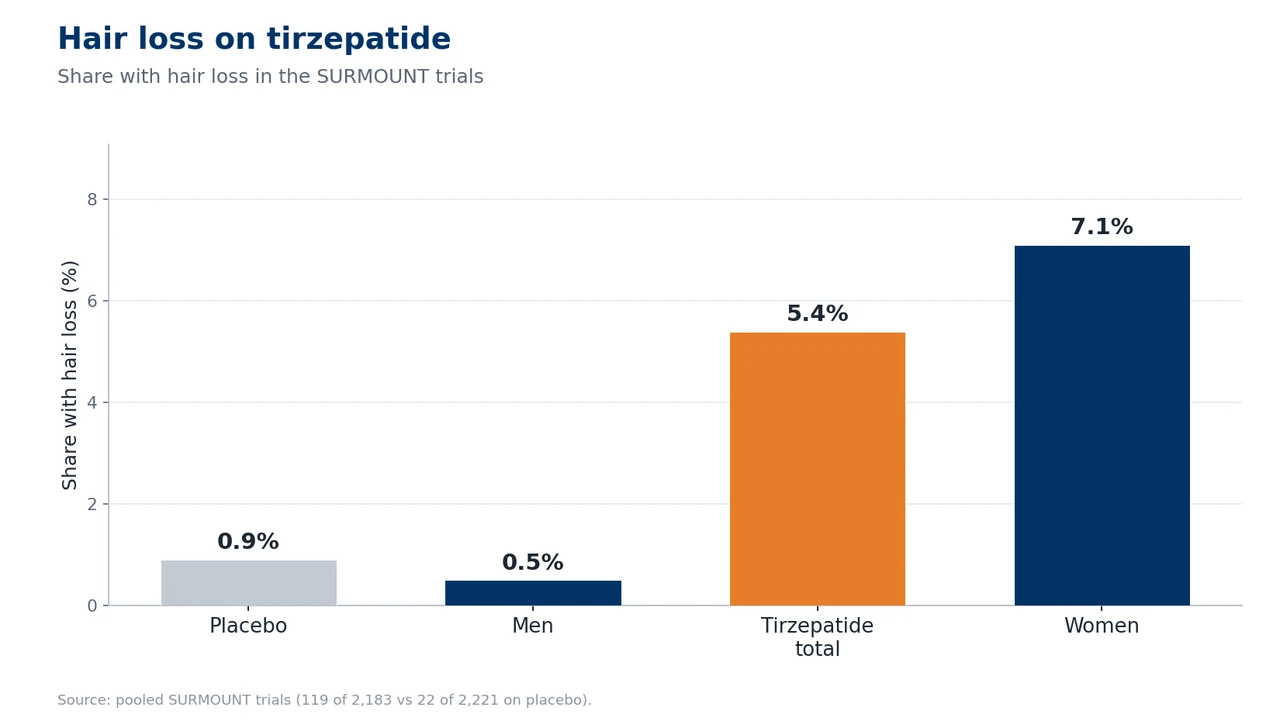
Tirzepatide is the most powerful weight-loss drug currently approved. Sold under the brands Mounjaro and Zepbound, it takes some patients past twenty per cent body-weight loss. That sheer force has a flip side nobody likes to talk about: a few months after starting, you suddenly find more hair in the brush, on the pillow, down the plughole. In the approval trials, roughly five per cent of participants reported hair loss, against around one per cent on placebo. In women it was as high as one in fourteen.
The key message first: in the vast majority of cases this is not a direct attack by the drug on your hair follicles. It is a telogen effluvium, triggered by rapid, significant weight loss. This page goes deep into the mechanics of the dual GIP/GLP-1 agonist, explains why tirzepatide carries the highest risk of the entire drug class, and shows the clear difference between Mounjaro (diabetes) and Zepbound (obesity). If you are looking for a specific brand, you will find the detail on our dedicated pages on Mounjaro and hair loss and on Zepbound and hair loss.
In short: tirzepatide and hair loss
Yes, tirzepatide (Mounjaro, Zepbound) can trigger hair loss, but almost never through the drug itself. The trigger is a telogen effluvium caused by rapid, significant weight loss. It is temporary and reversible: the hair grows back once your weight stabilises.
- Cause: the weight loss, not a toxic effect on the hair follicle. In the SURMOUNT trials, hair loss affected around 5 per cent (women 7.1 per cent, men 0.5 per cent).
- Temporary and reversible: the follicles stay intact, and regrowth begins after 6 to 12 months, provided there is no hereditary predisposition behind it.
- Highest risk of the class: up to 22.5 per cent weight loss. Zepbound (obesity) is more affected than Mounjaro (diabetes).
- When to see a doctor: if you notice bald patches, itching, or if there is no full regrowth after 12 months on a stable weight.
Do not stop the medication on your own simply because you are losing hair. Tirzepatide has real benefits for metabolism and weight, and the hair loss is usually temporary. If you are unsure whether there is also a hereditary component behind the shedding, have your hair assessed with a free hair analysis before you change anything.
Summary
- Does tirzepatide cause hair loss? The clinical evidence
- What does hair loss on tirzepatide look like?
- Why it happens: the mechanism behind tirzepatide
- The timeline: when does the hair loss arrive, and when does it come back?
- Mounjaro or Zepbound: why the brand changes the risk
- Who is most at risk?
- What is tirzepatide?
- Tirzepatide and hereditary hair loss: the unmasking
- What can I do about the hair loss?
- Does the hair grow back after tirzepatide?
- When does a hair transplant make sense?
- Tirzepatide compared with other GLP-1 drugs
- When you should see a doctor
- Frequently asked questions about tirzepatide and hair loss
- Conclusion: tirzepatide and hair loss
- Sources
Does tirzepatide cause hair loss? The clinical evidence
This question can be answered more clearly than for most drug side effects, because the data here are unusually good. Hair loss is explicitly listed for the obesity drug Zepbound in the official FDA label, specifically in section 6.1 (Clinical Trials Experience). That is the strongest class of evidence there is for a side effect: measured in randomised, controlled approval trials.
In the pooled data from the SURMOUNT trials, the frequency of alopecia across all doses was around 5 per cent, against roughly 1 per cent on placebo. The FDA label notes explicitly that the hair-loss reactions were “associated with weight reduction”. That single phrase is the key to the whole topic: it is the weight loss, not the drug itself.
SURMOUNT-1: the figures in detail
The approval trial SURMOUNT-1 (Jastreboff et al., NEJM 2022) studied 2,539 adults with obesity and without type 2 diabetes. For alopecia, a striking pattern emerged: tirzepatide 5 mg led to 5.1 per cent, 10 mg to 5.3 per cent and 15 mg to 4.9 per cent hair loss, against 0.9 per cent on placebo. The relative risk was therefore around five times higher.
What is conspicuous is what is missing here: a dose-response gradient. At 5, 10 and 15 mg the rate is practically the same. That is an important difference from semaglutide, where the risk clearly rises with the dose. The explanation fits the overall picture: it is not the amount of drug that decides things, but how much weight comes off in the end. We explore how this compares to pure GLP-1 drugs on our hub page on semaglutide and hair loss.
What the 2026 systematic review shows
A systematic review by Gupta and colleagues (Science Progress 2026) assessed 133 studies and included 24. The result: a 3.4-fold higher risk of alopecia on GLP-1 drugs compared with placebo. Tirzepatide and semaglutide were at the top. Across the SURMOUNT trials, hair loss affected 5.4 per cent of tirzepatide users (119 of 2,183) against 0.9 per cent on placebo (22 of 2,221).
The authors put it plainly: tirzepatide was, of all the GLP-1 drugs, “most frequently linked with telogen effluvium”, precisely because it produced the greatest weight loss. That brings us full circle to the mechanics, which we unpick further down.
FAERS reporting data: a contradictory signal
Being honest also means acknowledging the inconsistent data from the FDA’s reporting system, FAERS. A disproportionality analysis (Godfrey et al., JEADV 2025) found a reporting odds ratio of 1.73 for tirzepatide (95% CI: 1.42 to 2.09), and as high as 2.46 for semaglutide. A second, more recent analysis (Lee and Kim, DMRR 2026) found no significant signal for tirzepatide once it had been statistically adjusted. This divergence comes down to different models and time periods. An important point for context: spontaneous reporting data are weaker than controlled trials. The robust 5 per cent from the SURMOUNT trials remains the most reliable figure.
What does hair loss on tirzepatide look like?
The typical hair loss on tirzepatide is a telogen effluvium. That means: diffuse and evenly spread across the whole scalp, with no bald patches and no recognisable pattern. You do not lose a single region such as the temples; instead you notice that your hair looks thinner and less dense overall. It shows up above all in more hair in the brush, in the shower and on the pillow. Many people describe hair coming away “in handfuls” when they wash it.
This is clearly distinct from androgenetic alopecia, the hereditary form of hair loss. That follows a pattern: a receding hairline and crown thinning in men, and thinning along the central parting in women. It develops gradually over months and years, not acutely. This distinction is crucial, because it determines the outlook. You can read more about the hereditary type in our article on androgenetic alopecia.
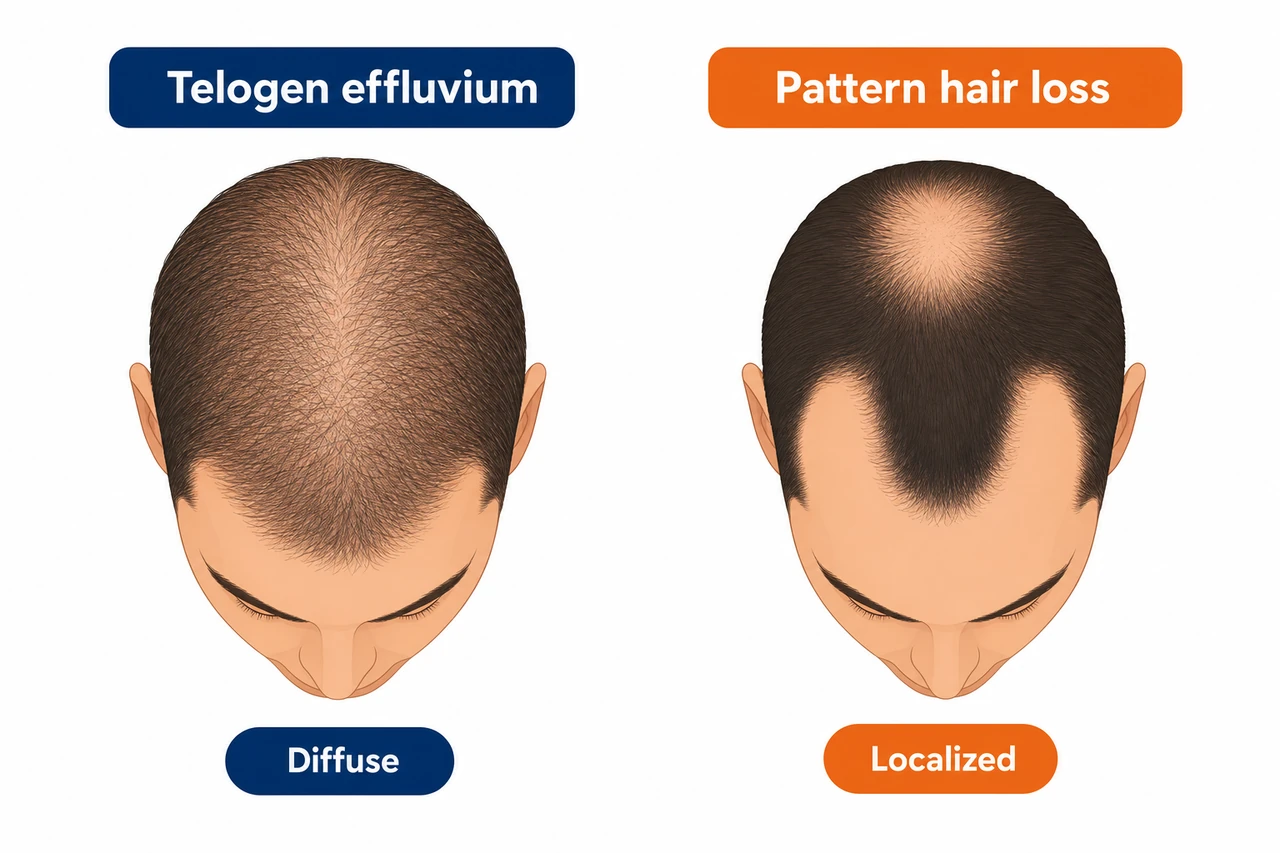
| Feature | Telogen effluvium (TE) | Androgenetic alopecia (AGA) |
|---|---|---|
| Pattern | Diffuse, whole scalp | Receding hairline, crown, parting |
| Onset | Acute, 2 to 4 months after the trigger | Gradual, progressive |
| Reversibility | Yes, follicles intact | No, miniaturisation permanent |
| Dermoscopy | No miniaturisation | Visible miniaturisation |
Which type is it in your case? This is the fork in the road that decides your next step
This is the reversible, normal case and needs no hair transplant. The follicles are merely resting. Your plan: patience over 6 to 12 months, keep an eye on protein and iron (check your ferritin) and ease off the pace of the weight loss. If in doubt, a hair analysis will confirm whether it really is only a telogen effluvium.
If the weight loss unmasks an androgenetic alopecia that was already there, that part will not grow back on its own. This is the case that needs a permanent solution. Here it is worth getting an accurate diagnosis before you treat anything.
Not sure which type it is? That is precisely the most important question. A free hair analysis separates a reversible telogen effluvium from a hereditary alopecia that needs treatment, before you rush to stop an effective therapy or worry unnecessarily about a transplant.
Why it happens: the mechanism behind tirzepatide
To understand why tirzepatide in particular carries the highest hair-loss risk of the entire drug class, you need to bring two things together: what the drug does in the body, and how the hair cycle responds to stress.
The dual GIP/GLP-1 agonist: stronger than anything else
Tirzepatide is the first and so far only approved member of a new class: a dual agonist that activates two receptors at once. First, the GLP-1 receptor (glucagon-like peptide-1), just like semaglutide. Second, the GIP receptor (glucose-dependent insulinotropic polypeptide) on top. This combination is known as a twincretin. The GLP-1 component slows gastric emptying, inhibits glucagon and dampens appetite via the satiety centre in the hypothalamus. The GIP component boosts insulin secretion synergistically and improves insulin sensitivity in fat and muscle tissue.
The result of this twin action is weight loss that outstrips pure GLP-1 drugs: up to 22.5 per cent of body weight on 15 mg in SURMOUNT-1, against around 15 per cent on semaglutide 2.4 mg. It is precisely this superiority at weight loss that is also the root of the higher hair-loss risk. It is not the GIP receptor attacking the hair follicle. It is the sheer amount of weight lost in a short time.
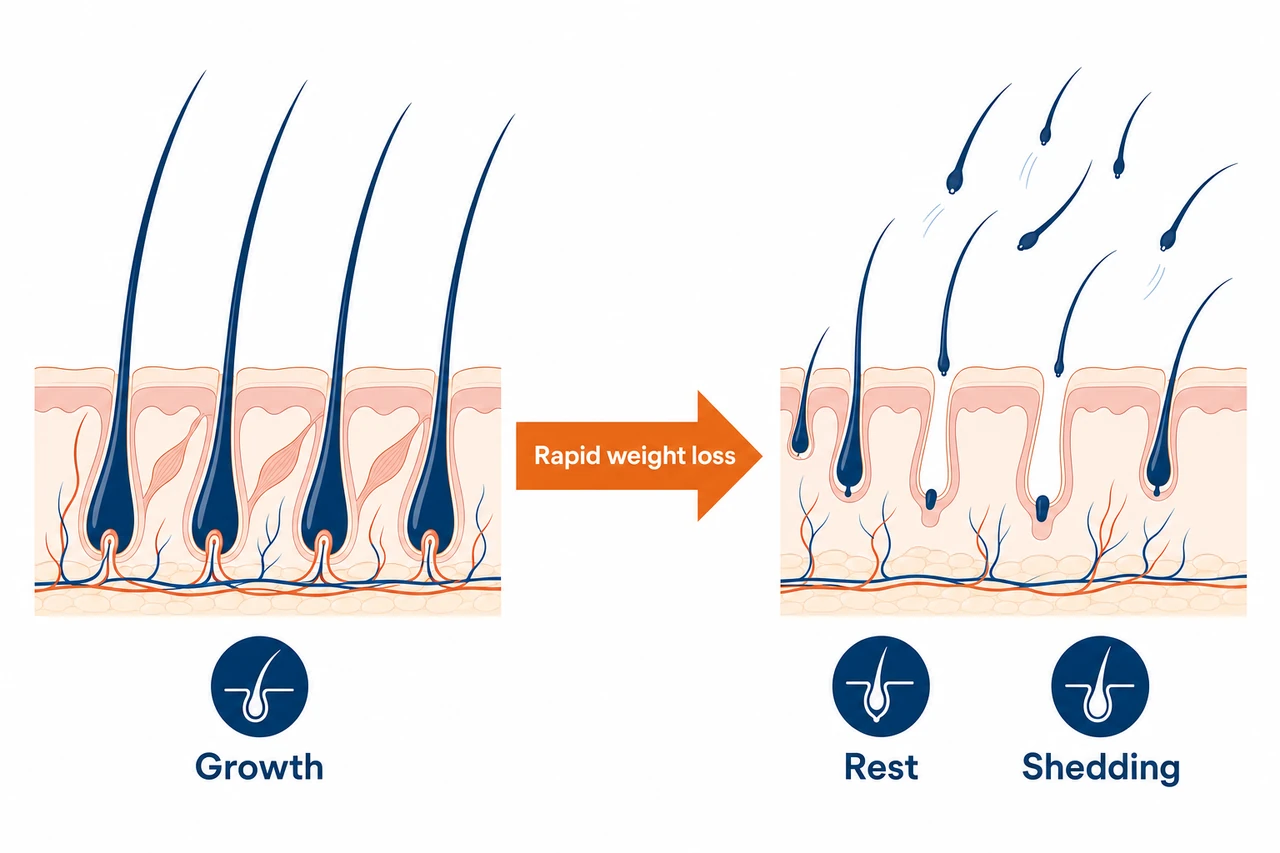
Telogen effluvium from rapid weight loss
This is the heart of it. When the body loses a lot of weight in a short space of time, it enters a state of metabolic and physiological stress. It prioritises the vital organs and dials back functions that are not essential to life. Hair growth is one of them. As a result, large numbers of hairs switch prematurely from the active growth phase (anagen) into the resting phase (telogen). Up to 70 per cent of growing hairs can tip into the resting state in this way.
The decisive point for the timing: a hair that moves into the resting phase does not fall out until around 2 to 4 months later. That is why you never notice the hair loss the moment you start, but with this characteristic delay. We explain how the whole process works in detail in our article on the hair growth cycle. The direct link between the scale of the weight loss and the risk is measurable in numbers: at more than 20 per cent weight loss the alopecia rate rose to 5.3 per cent, while at less than 20 per cent it was only 2.5 per cent.
Nutrient deficiencies as an accelerant
Tirzepatide suppresses appetite so strongly that many patients unintentionally eat too little. On top of that, the drug markedly slows gastric emptying, which can temporarily alter the absorption of individual micronutrients. Less food and sluggish digestion compound the stress on the hair follicles through several routes:
- Protein deficiency. Hair is around 90 per cent keratin. If protein intake falls below 0.8 g per kilogram of body weight per day, the risk of a telogen effluvium doubles.
- Iron deficiency. Iron is a cofactor of a key enzyme in DNA synthesis within the hair matrix cells. A 2025 study found iron deficiency in 88.4 per cent of Mounjaro users with hair loss. The target is a ferritin level above 70 ng/mL.
- Zinc deficiency. Patients with chronic telogen effluvium showed significantly lower zinc levels than controls (49.91 versus 60.53 µg/dL).
- HPA stress axis. Rapid weight loss raises the stress hormone cortisol, which further inhibits hair growth via CRH receptors.
Vitamin D status is often mentioned too, but the data on it is contradictory. Vitamin D is at best a possible cofactor, not the main mechanism.
The paradoxical flip side: sometimes tirzepatide helps the hair
As clear as the trend towards hair loss is, there is a counter-movement. Tirzepatide improves insulin sensitivity even more than semaglutide. In people with marked insulin resistance, that can actually slow hereditary hair loss, because insulin resistance promotes the production of DHT, the driver of androgenetic alopecia. A single documented case (Gordon et al., JAAD Case Reports 2024) showed a measurable improvement in hair density in a 57-year-old man with insulin resistance after twelve months on tirzepatide. An important caveat: that is a single case report, not proof of effect. Tirzepatide is in no way a hair-growth treatment and should never be used for that purpose. The effect is therefore two-way and depends on the individual: through weight loss, tirzepatide can cost you hair; in marked insulin resistance it can, in rare cases, indirectly favour hair density.
The timeline: when does the hair loss arrive, and when does it come back?
Hair loss on tirzepatide follows a predictable course. If you know what to expect, you will not panic at the first shedding and can better judge whether everything is within the expected range.

| Phase | Period | What happens |
|---|---|---|
| Initiation | Week 1 to month 3 | Dose escalation, significant weight loss. Hairs switch unnoticed into the resting phase, with no visible loss yet. |
| Shedding | Month 2 to 6 | Visible hair loss, usually peaking in months 4 to 6. The active phase lasts several weeks to around 3 months. |
| Stabilisation | Month 6 to 9 | Weight loss slows, stress eases. The first new anagen hairs begin to grow. |
| Regrowth | Month 6 to 18 | Cosmetically visible regrowth. Full recovery takes up to 12 to 18 months, provided your weight is stable. |
An important note on the trigger: it is not only starting the therapy that can set off a new telogen effluvium, but every dose increase too, especially if your weight then drops quickly again. The standard schedule raises the dose every four weeks, from 2.5 mg through 5, 7.5, 10 and 12.5 mg up to the maintenance dose of 15 mg.
Mounjaro or Zepbound: why the brand changes the risk
Mounjaro and Zepbound contain exactly the same active ingredient, tirzepatide, in the same doses. Even so, their hair-loss risk differs, and the reason is the indication, not the substance.
Used for blood-sugar control in type 2 diabetes. The weight loss is smaller and slower, around 11 kg on 15 mg over 40 weeks in the SURPASS trials. That is why alopecia was only added later, in February 2025, in section 6.2 (Postmarketing) of the FDA label. Detail on the Mounjaro page.
Approved for chronic weight management. The weight loss is dramatic, up to 22.5 per cent over 72 weeks. The telogen effluvium appears earlier and more strongly. Alopecia is listed directly in section 6.1 (Clinical Trials) of the FDA label. Detail on the Zepbound page.
The rule of thumb could not be simpler: the more weight comes off in a short time, the higher the risk of a telogen effluvium. Someone taking tirzepatide for diabetes who loses weight moderately is less at risk than someone losing 25 kilograms in a year on Zepbound. Both groups, however, benefit from the same prevention.
Who is most at risk?
The risk is not evenly distributed. These factors markedly increase the likelihood of noticeable hair loss on tirzepatide:
- The extent of the weight loss. By far the single biggest factor. More than 20 per cent weight loss means roughly double the risk compared with less than that.
- Being female. In the Zepbound trials, women were massively over-represented at 7.1 per cent against just 0.5 per cent for men. Hormonal fluctuations and lower iron stores play a part. A 2025 Canadian study found a significantly higher risk for women, but not for men.
- A fast titration pace. Anyone who escalates the dose aggressively and loses weight rapidly as a result accumulates more triggers for a telogen effluvium.
- Pre-existing nutrient deficiencies. Low ferritin, zinc deficiency or too little protein noticeably raise the risk.
- Genetic predisposition. In analyses, more than 90 per cent of reported cases already had a history of hair loss. Tirzepatide can unmask a previously invisible hereditary predisposition.
What is tirzepatide?
Tirzepatide is a dual GIP/GLP-1 receptor agonist made by Eli Lilly, given as a once-weekly subcutaneous injection. It is the first approved drug of its class, a so-called twincretin. It is marketed under two brand names with an identical active ingredient but different indications:
- Mounjaro (approved May 2022): for blood-sugar control in type 2 diabetes mellitus, alongside diet and exercise.
- Zepbound (approved November 2023): for chronic weight management in obesity, or in overweight with a related condition, and since 2024 additionally for obstructive sleep apnoea.
In the pivotal trials, tirzepatide 15 mg achieved −22.5 per cent body weight in obesity alone (SURMOUNT-1) and clearly outperformed semaglutide head to head on diabetes weight loss (SURPASS-2). That potency is the medical advantage and, at the same time, the cause of the raised hair-loss risk.
Tirzepatide and hereditary hair loss: the unmasking
This is where it becomes crucial for many people. A telogen effluvium is temporary and reversible. But rapid weight loss can bring a previously hidden androgenetic alopecia to the surface. The hereditary predisposition often runs unnoticed beneath the surface for years. Sudden, heavy shedding can effectively pull the curtain off this latent AGA: where dense hair once camouflaged the slow thinning, the hereditary loss becomes visible all at once after the telogen effluvium.
In the large TriNetX cohort study (Vidal/Akiska et al., JAAD International 2026) of 547,993 matched adults, androgenetic alopecia on GLP-1 drugs was raised by a factor of 1.64 after 12 months. Patients typically only report a receding hairline or parting thinning after starting tirzepatide, even though the predisposition was there all along. How far advanced a hereditary loss is can be classified using the Norwood-Hamilton scale. The wider role that hormones play here is explored in our article on hormones and hair.
The practical consequence: pure telogen effluvium grows back within 12 months. An unmasked AGA does not; it needs its own treatment. In practice there is often a combination of the two. In that case the rule is: wait out the TE component first, then treat the AGA in a targeted way.
What can I do about the hair loss?
A telogen effluvium cannot be prevented one hundred per cent, but the risk can be cut significantly. The main levers are diet and pace.
The most effective protective measures:
- ✅ Enough protein. Target: 1.2 to 1.6 g per kilogram of body weight a day, at least 60 g. Spread it over 3 to 4 meals. Tirzepatide blunts hunger so strongly that under-eating is the real main risk.
- ✅ Check your micronutrients. Have ferritin (target above 70 ng/mL), zinc, vitamin D, vitamin B12 and thyroid levels checked before starting therapy and every 3 to 6 months.
- ✅ Correct iron deliberately. If ferritin is below 40 ng/mL, supplement after speaking to your doctor, ideally with vitamin C.
- ✅ Ease off the pace. If weight loss is very rapid, above 1.5 kg per week, postpone the next dose increase with your doctor. Target: 0.5 to 1 kg per week.
- ⚠️ No high-dose biotin. Biotin does not help on a normal diet and can skew lab tests, with documented errors in troponin readings, for example. The FDA warns against it explicitly.
Does the hair grow back after tirzepatide?
If the shedding is already under way, there are several levers to pull. The most important one remains tackling the cause: stabilise your weight and correct any nutrient deficiencies.
- Topical minoxidil 5%. Approved for androgenetic alopecia, and also used off-label for telogen effluvium. An open-label study showed a clear improvement in hair density after 24 weeks. At the start the hair loss can briefly increase, which is to be expected. More on this in our article on minoxidil for hair loss.
- Oral low-dose minoxidil. Off-label, prescribed only by experienced doctors. In studies, a large proportion of patients showed improvement or stabilisation.
- Correct nutrient deficiencies at source. Iron for low ferritin, zinc only where a deficiency is proven, vitamin D where levels are low.
- PRP (platelet-rich plasma). A 2024 meta-analysis showed improvements in hair density and the pull test. For GLP-1-specific TE the evidence is extrapolated, not studied directly.
What does not help: high-dose biotin without a proven deficiency. The only sound randomised study found no difference from placebo. The line to remember: biotin does nothing, but it can skew your lab values.
In patients who lose hair on Mounjaro or Zepbound, the trigger is almost always the rapid weight loss, not the drug itself. The good news: such hair usually grows back once the weight stabilises and the diet is right. What matters is establishing early on whether a hereditary predisposition is also at play. That distinction is exactly what should come first, not the hasty discontinuation of a therapy that makes medical sense.
Dr. Balwi, Medical Director at Elithair
When does a hair transplant make sense?
The clear message first: for a pure telogen effluvium, a hair transplant is neither necessary nor sensible. The follicles are intact, they are merely resting. They grow back on their own. A transplant during an active shedding phase would even be counterproductive, because the transplanted hairs land in the same stressed environment and can also tip into the resting phase.
A transplant only becomes sensible if, after around 12 months on a stable weight and with good nutrition, there is still no full regrowth. In that case there is usually an unmasked or pre-existing androgenetic alopecia behind it. The prerequisites are a stable donor area and no more active shedding. Elithair works with the DHI and FUE methods and complements them with NEO FUE. The transplanted hair comes from the hormone-resistant donor area and therefore does not fall out again.
The first step is always the diagnosis. A free hair analysis establishes whether there is still a waiting telogen effluvium behind your hair loss, or already an AGA that needs treatment. If you are considering the step towards treatment, you will find all the information on our hair transplant page.
Tirzepatide compared with other GLP-1 drugs
Where does tirzepatide sit in the risk ranking of the weight-loss jabs? The table below ranks the main drugs by clinical trial incidence, FDA label status and magnitude of weight loss.
| Drug / brand | Indication | Alopecia in trials | FDA label | Notable point |
|---|---|---|---|---|
| Tirzepatide / Zepbound | Obesity | 4.9 to 5.3% vs 0.9% placebo | Section 6.1 (Clinical Trials) | Strongest weight loss of all GLP-1s; women 7.1% |
| Tirzepatide / Mounjaro | Diabetes | ~ 4.9 to 5.7% in meta-analyses | Section 6.2 (Postmarketing, 2025) | Slower weight loss, later label entry |
| Semaglutide / Wegovy | Obesity | 3.3% vs 1% placebo | Section 6.1 (Clinical Trials) | Dose-dependent; women 4% |
| Semaglutide / Ozempic | Diabetes | Not listed in 6.1 | Postmarketing only | Lower maximum dose, slower titration |
The seemingly paradoxical situation: in the approval trials, tirzepatide (5%) sits slightly above semaglutide/Wegovy (3%), while in the FAERS reporting system it is the other way round. The reason: FAERS depends heavily on reporting behaviour, and tirzepatide is the newer drug with fewer reports overall. The controlled trial data are more robust. The head-to-head comparison of tirzepatide versus semaglutide is the subject of our semaglutide hub page.
When you should see a doctor
A diffuse telogen effluvium on tirzepatide is usually harmless and temporary. Certain warning signs, though, should be looked into:
- See a doctor within a few days: round, bald patches (suspected alopecia areata), redness, itching, burning or crusting on the scalp (suspected scarring alopecia, irreversible if untreated), or massive loss of more than 200 to 300 hairs a day over weeks.
- See a dermatologist within 4 to 8 weeks: if the telogen effluvium persists for more than 6 months without improvement, if the diagnosis is unclear, or if a co-existing androgenetic alopecia is suspected.
- After 12 months without full regrowth: a free hair analysis at Elithair to establish whether it is still a matter of waiting or whether a surgical option is now on the table.
Which specialist you need depends on the question. For diagnosing the hair loss (trichogram, dermoscopy, distinguishing TE from AGA), a dermatologist is the right port of call. If the point is to adjust the dose or titration pace, that belongs with the treating doctor or endocrinologist managing your tirzepatide therapy. Important in every case: do not stop tirzepatide on your own. Always discuss any changes with your treating doctor.
Frequently asked questions about tirzepatide and hair loss
Conclusion: tirzepatide and hair loss
Tirzepatide can cost you hair, and the data shows this clearly: around 5 per cent in the approval trials, more in women. But the cause is almost always a telogen effluvium driven by the strongest weight loss of the entire drug class, not a direct attack on the hair follicle. That is precisely what makes the hair loss reversible in most cases. Zepbound carries a higher risk than Mounjaro here, because the weight loss is more dramatic. Anyone who watches their protein, checks their nutrients and keeps an eye on the pace of the weight loss can cut the risk noticeably. And anyone who sees no full regrowth after 12 months should have the true cause investigated, rather than hastily abandoning an effective therapy.
Sources
- Jastreboff AM et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). NEJM 2022. NEJM
- Zepbound® FDA Prescribing Information, section 6.1, NDA 217806, Eli Lilly, 2024. FDA
- Mounjaro® FDA Prescribing Information sNDA 215866s031, section 6.2 (Postmarketing), Feb 2025. FDA
- Gupta AK, Teasell EM, Economopoulos V, Mirmirani P. GLP-1 therapies and hair loss: A systematic review. Science Progress 2026. DOI
- Godfrey H et al. Alopecia associated with semaglutide and tirzepatide: FAERS disproportionality analysis. JEADV 2025. PubMed
- Vidal SI, Akiska YM et al. Increased Risk of Hair Loss with GLP-1 Receptor Agonists: TriNetX Cohort Study. JAAD International 2026. PMC
- Gordon ER et al. Treatment of insulin resistance with tirzepatide leading to improvement of hair loss. JAAD Case Reports 2024. PMC
- Rojas Lopez RF et al. Alopecia as an Emerging Adverse Effect of GLP-1 Receptor Agonists: A Scoping Review. Cureus 2025. PMC
- StatPearls. Telogen Effluvium. NIH/NCBI, 2024. NCBI
- Pugliese et al. Biotin for Hair Loss: Systematic Review. JCAD 2024. PubMed
- FDA. Biotin (Vitamin B7): Safety Communication. 2019. FDA
- AAD. How can GLP-1 drugs affect my skin, hair, and nails? 2026. aad.org
This article is for information only and does not replace medical advice. Never stop tirzepatide (Mounjaro, Zepbound) on your own, and discuss any change to your therapy with a qualified doctor. If your hair loss persists, you should seek a professional diagnosis.

Dr. Imad Moustafa
Hair transplant specialist