
You have been injecting semaglutide for a few months, the weight is finally coming off, and suddenly there are noticeably more hairs in the drain each morning and on your pillow. The worry kicks in right away: is the weight-loss shot now costing me my hair? Thousands of patients taking Wegovy, Ozempic or Rybelsus ask themselves exactly this. And it is a fair question, because hair loss really does appear in the Wegovy patient information.
The good news first: in the vast majority of cases the active substance semaglutide is not the real problem, the speed at which you are losing weight is. The hair loss is almost always a telogen effluvium (a temporary, diffuse shedding caused by many follicles entering their resting phase early), a temporary and reversible reaction to rapid weight loss. On this page we explain the mechanism of the drug in detail, put the real figures from the approval trials into context, show the difference between Ozempic and Wegovy, and say plainly when hair loss is harmless and when you should take a closer look.
In short: does semaglutide cause hair loss?
Yes, semaglutide can trigger hair loss, but almost always only indirectly. The culprit is not the drug itself, it is the rapid weight loss, which sets off a telogen effluvium: a temporary, diffuse shedding. This usually resolves on its own once your weight stabilizes, so hair loss alone is rarely a reason to stop treatment.
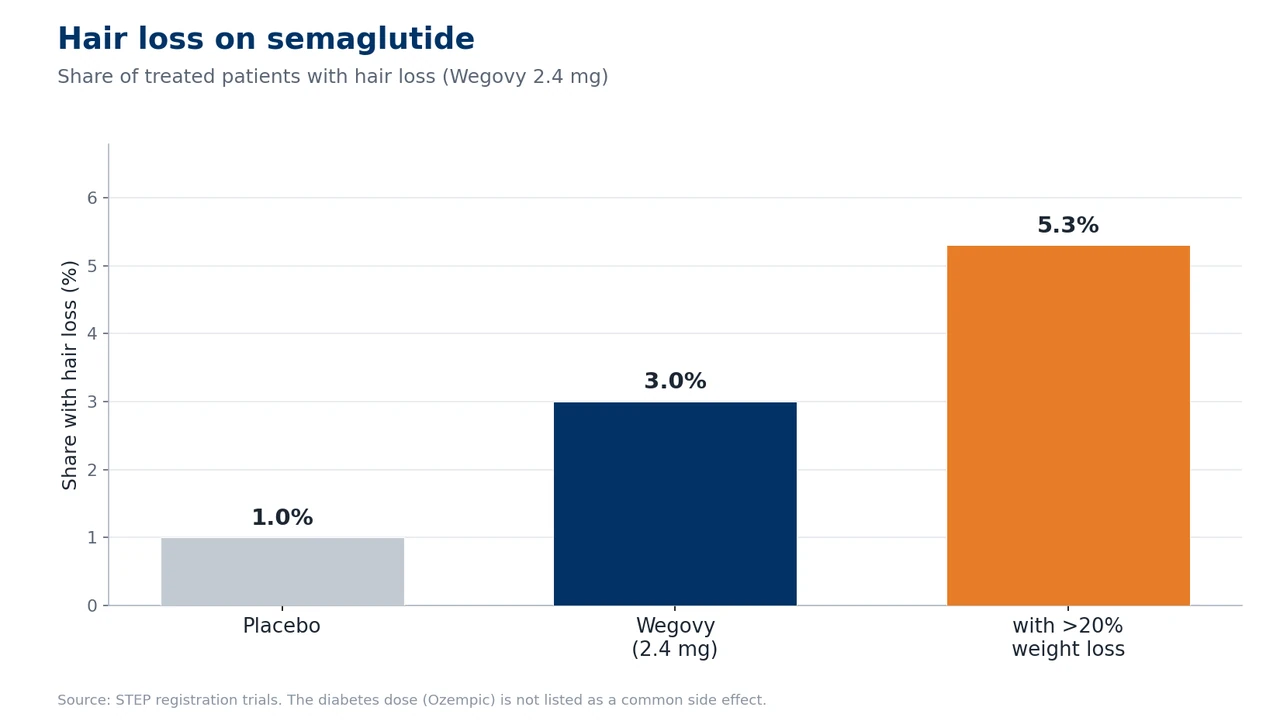
- Cause: the rapid weight loss, not a toxic effect of the drug on the hair root. In the Wegovy trials (2.4 mg) around 3% of patients were affected, compared with 1% on placebo.
- Temporary and reversible: once your weight stabilizes, the hair typically grows back within 6 to 12 months.
- Risk depends on how fast you lose weight: losing more than 20% of your body weight nearly doubles the risk. That is why Ozempic (lower dose) affects fewer people than Wegovy.
- When to see a doctor: with bald patches, no regrowth after 12 months, or a patterned loss alongside a family history (suggesting hereditary hair loss).
If you are losing hair on semaglutide, that is in most cases no reason to stop treatment. What matters more is reading the cause correctly and knowing the handful of levers you can pull to lessen the loss. That is exactly what we will work through, step by step.
Summary
- Does semaglutide cause hair loss? The clinical evidence
- How does the hair loss on semaglutide show up?
- Why does it happen? How semaglutide works
- Timeline: when does the hair loss start, and when does it stop?
- Who is most at risk?
- What exactly is semaglutide? Brands and indications
- Semaglutide and hereditary hair loss: the unmasking problem
- What can I do about hair loss on semaglutide?
- Does hair grow back after semaglutide?
- The Elithair approach: when does a hair transplant make sense?
- Semaglutide compared with other GLP-1 drugs
- When should you see a doctor? The warning signs
- Frequently asked questions about semaglutide and hair loss
- The verdict: does semaglutide cause hair loss?
- Sources
Does semaglutide cause hair loss? The clinical evidence
The most reliable source is the official Prescribing Information from the FDA. And here the most important quirk of this drug shows up immediately: semaglutide is sold in three very different products, and only one of them lists hair loss in its label at all.
- Wegovy (semaglutide 2.4 mg, weekly, for obesity): alopecia is listed in section 6.1 of the FDA Prescribing Information as a known side effect. Incidence is 3% in adults (2.4 mg) versus 1% on placebo. In adolescents aged 12 and over it reaches 4% versus 0%. The FDA explicitly notes that the hair loss was associated with weight reduction.
- Ozempic (semaglutide 0.5 to 2.0 mg, weekly, for type 2 diabetes): hair loss is NOT listed in section 6.1 of the FDA label, at most as a post-marketing report with no frequency given. The reason lies in the much smaller weight loss seen in the diabetes indication.
- Rybelsus (semaglutide 7 to 14 mg, oral, daily, for type 2 diabetes): again, no hair loss in the label. In the PIONEER trial program the weight loss was around 4 kg, too little to trigger a telogen effluvium.
Across the obesity studies, the Wegovy label classes alopecia as a common adverse reaction, affecting at least 1 in 100 patients treated, with a rate of 2.5% versus 1.0% on placebo. The important addition: the events were mostly mild, and most patients recovered while still on treatment.
What the STEP trials show
The approval of semaglutide for weight loss rests on the STEP trial program. In STEP 1 (Wilding et al., NEJM 2021, n=1,961, 68 weeks) the mean weight loss was −14.9%, and alopecia occurred in around 3% versus 0.9% on placebo. STEP 5, run over 104 weeks, confirmed the picture with −15.2% weight loss and roughly 3.2% alopecia. One detail within these data is decisive: patients who lost more than 20% of their body weight showed an alopecia rate of 5.3%, against only 2.5% in those who lost less than 20%. It is the extent of the weight loss that drives the risk, not the substance itself.
FAERS pharmacovigilance and real-world data
There are signals outside the approval trials too. An analysis of the FDA’s adverse-event database FAERS, the system in which doctors and patients report suspected side effects, found a reporting odds ratio of 2.46 for semaglutide (Godfrey et al., JEADV 2025) (95% CI: 2.14 to 2.83). The reporting odds ratio shows how much more often a side effect is reported for a drug than for others, so a value above 1 is a warning sign. This is the first solid pharmacovigilance signal for the weekly GLP-1 receptor agonists. A large real-world cohort study using the TriNetX database (n=547,993 matched patients) found an increased risk of non-scarring alopecia at 12 months, with an adjusted odds ratio of 1.40. In a meta-analysis of 24 studies (Gupta et al., Science Progress 2026, more than 84,000 patients), the alopecia risk on GLP-1 therapies was roughly 3.4 times higher than on placebo.
How does the hair loss on semaglutide show up?
The typical hair loss on semaglutide is a diffuse, even thinning across the whole scalp. There are no clearly defined bald patches. In practice, most people simply notice far more hair in the brush, in the shower drain and on the pillow. Instead of the normal 50 to 100 hairs a day, 150 or more come out for a while. When you put your hair up it feels thinner, and the part looks wider than before. This pattern is exactly what is typical of a telogen effluvium and sets it apart from a patterned diffuse hair loss with a clear progression.
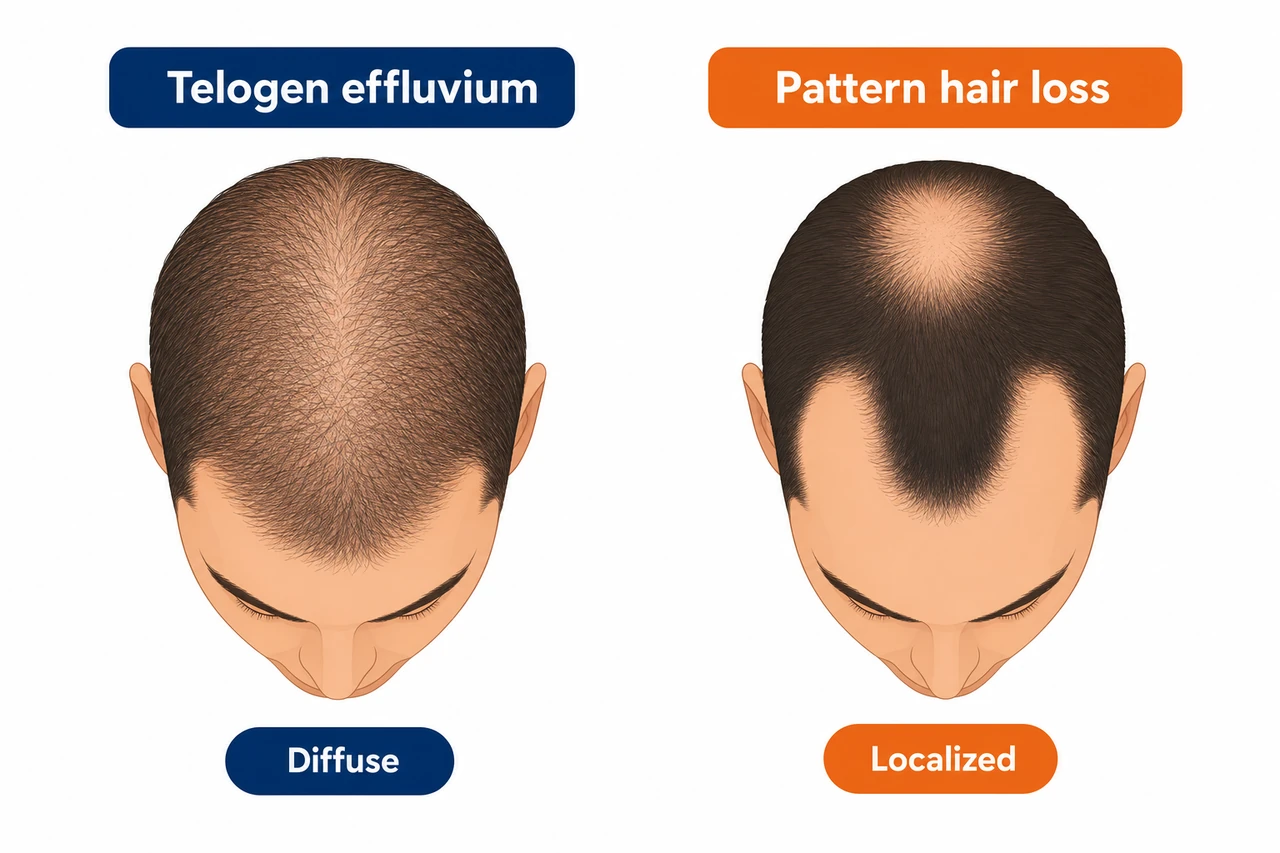
This needs to be distinguished from androgenetic alopecia (AGA), the hereditary, hormone-driven hair loss with its characteristic pattern. In men it shows up at the temples and on the crown following the Hamilton-Norwood pattern, in women as thinning along the part in the so-called Christmas-tree pattern. Interestingly, in a cohort of 283 GLP-1 users (Burke et al., JAAD 2025) it was not telogen effluvium but AGA that was the most commonly diagnosed subtype, in 19 of 35 cases. That suggests semaglutide unmasks an AGA in some people that was already present but until then invisible.
In very rare individual cases, alopecia areata has also been described, that is round, well-defined bald patches of autoimmune origin. A causal link with semaglutide has not been proven, but if you notice patchy loss you should see a dermatologist promptly.
Why does it happen? How semaglutide works
To understand the hair loss properly, you need to know what semaglutide actually does in the body. Semaglutide is a glucagon-like peptide-1 receptor agonist, GLP-1 RA for short. It mimics the body’s own gut hormone GLP-1 and activates its receptors in the pancreas, the brain and other organs. The result: insulin release is increased in a glucose-dependent way, gastric emptying is slowed, and, above all, appetite is dampened in the hypothalamus. You eat less, you feel full for longer, and your weight comes down. On Wegovy 2.4 mg the average loss is −14.9% over 68 weeks, and in some patients as much as 25%.
And it is precisely this rapid weight loss that is the real trigger for the hair loss, not the drug directly. The body reads a fast, marked drop in weight as physiological stress. It prioritizes vital organs and diverts energy and nutrients away from functions that are not essential for survival, and hair growth is one of those. The result is a telogen effluvium.
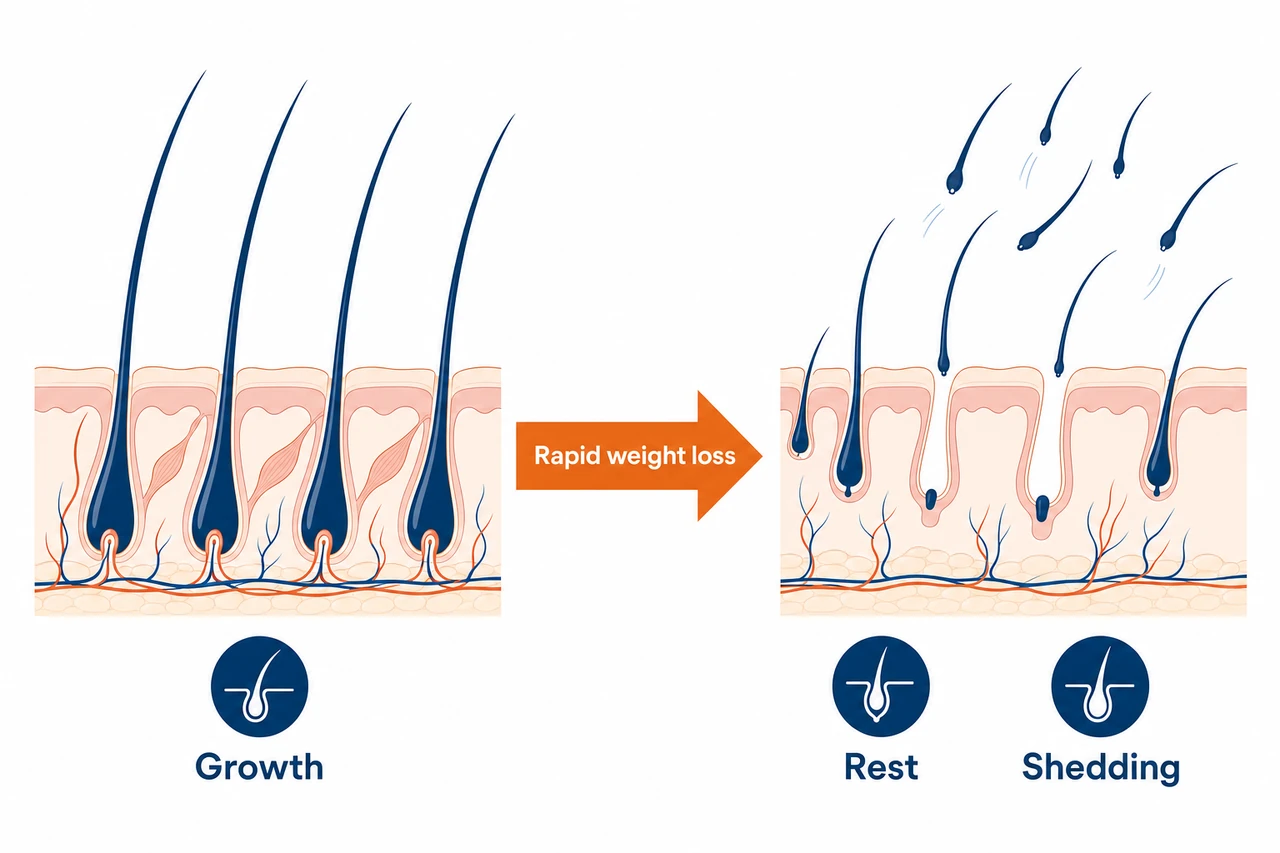
In detail it works like this. Normally 90 to 95% of your scalp follicles are in the active growth phase (anagen) and only 5 to 10% in the resting phase (telogen). Under severe stress the body can push up to 70% of the anagen hairs into the telogen phase prematurely, all at once. The HPA axis (the hormonal stress axis between the brain and the adrenal glands) plays a central role here: raised cortisol and corticotropin-releasing hormone (CRH) drive the follicles into rest. A characteristic delay of around 2 to 3 months sits between the trigger and the visible shedding, because the hairs sent into telogen only fall out at the end of their resting phase. Once you understand this hair growth cycle, it becomes obvious why the loss only appears months after starting treatment.
Nutrient deficiencies as an amplifier
Because you eat less on semaglutide, deficiencies can develop that make the telogen effluvium worse. Three are particularly relevant:
- Protein: hair is roughly 90% made up of the structural protein keratin. A protein intake below 0.8 g/kg/day is associated with a doubling of the TE risk, and when your appetite is suppressed it is all too easy to fall short.
- Iron and ferritin: iron is a cofactor of ribonucleotide reductase, the rate-limiting enzyme of DNA synthesis in the fast-growing hair matrix cells. In a controlled study, the mean ferritin level in patients with TE was 24.3 ng/mL versus 45.6 ng/mL in healthy controls.
- Zinc: essential for protein synthesis in the follicle. In chronic TE, significantly lower zinc levels have been measured (49.9 versus 60.5 µg/dL).
For vitamin D the data are contradictory. The vitamin D receptor regulates the hair cycle, but not every study finds lower levels in TE patients. We therefore do not present a vitamin D deficiency as a confirmed cause.
No direct follicle-toxic effect of the drug
This is the key distinction, and it is reassuring: all the current review articles agree that a direct cytotoxic effect of semaglutide on the hair follicles has not been proven. GLP-1 receptors have indeed been detected in the hair follicles of mice, but solid evidence of functional GLP-1 receptors in human hair follicles is still awaited. Put another way: semaglutide does not poison your hair. Through the weight loss it triggers a temporary stress reaction. From this follows an important practical consequence. Hair loss alone is usually no reason to stop treatment, because the medical benefit in obesity and type 2 diabetes outweighs it.
How it unfolds, step by step:
- ➊ Semaglutide dampens appetite, you lose a lot of weight (on average −15%, sometimes up to −25%).
- ➋ The rapid weight loss means physiological stress plus a calorie deficit.
- ➌ Nutrient deficiencies develop: protein, ferritin and zinc all drop.
- ➍ Cortisol and CRH rise, and up to 70% of the follicles enter the resting phase.
- ➎ After a latency of 2 to 3 months, diffuse hair loss appears.
- ➏ Reversible after 6 to 12 months. No direct follicle damage from the drug.
Timeline: when does the hair loss start, and when does it stop?
The dose escalation of semaglutide is closely tied to the hair-loss timeline. Wegovy is titrated up over 16 weeks: 0.25 mg, then 0.5 mg, 1.0 mg, 1.7 mg and finally 2.4 mg, in 4-week steps. With each dose increase the weight loss speeds up. That is why the shedding phase, the period of markedly increased loss of the hairs previously sent into rest, often begins after the first significant dose increase. Ozempic escalates more slowly and only up to a maximum of 2.0 mg, which goes some way to explaining its smaller weight loss and the absence of a label signal.
| Phase | Period | What happens |
|---|---|---|
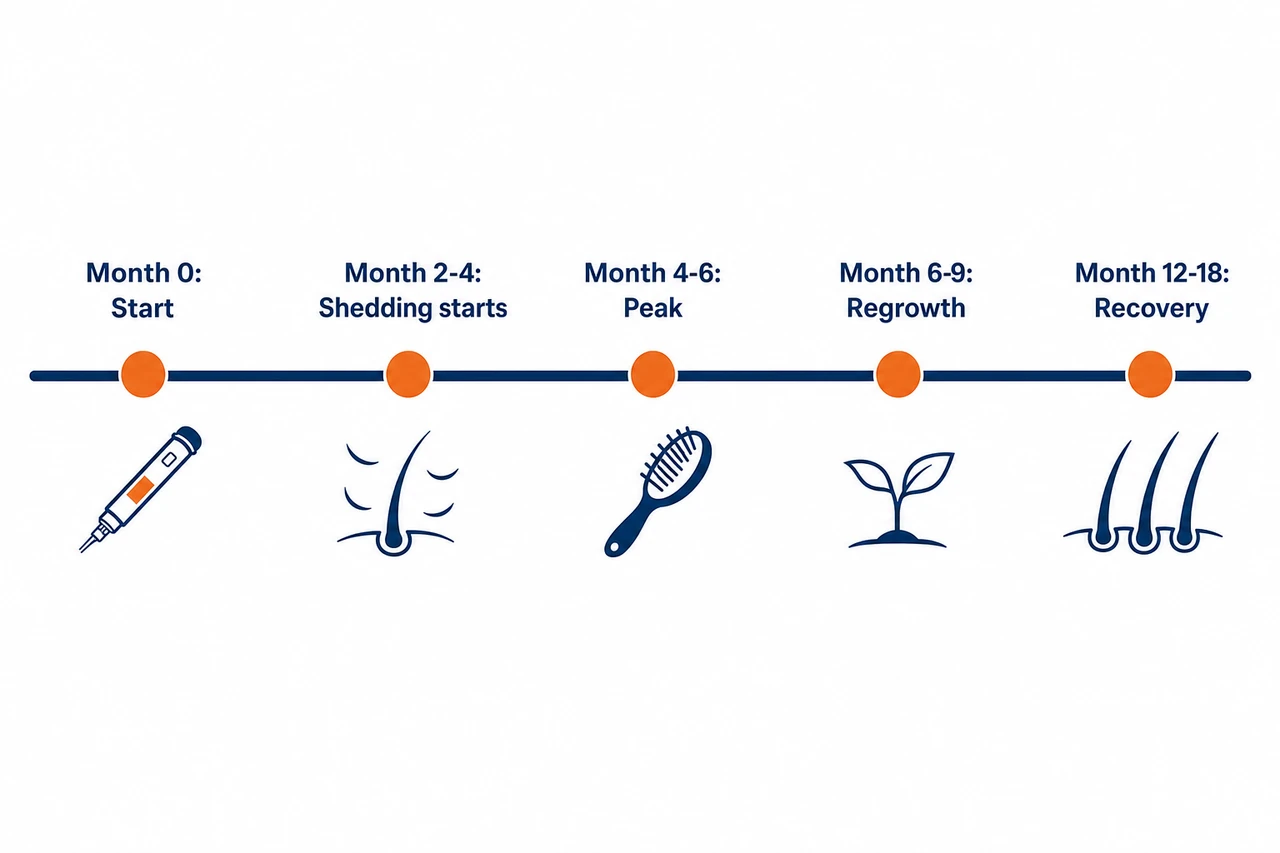
| Latency | Start to month 2–4 | Weight loss begins. Follicles quietly enter the telogen phase. No visible loss yet. |
| Shedding begins | Month 2–4 | Suddenly far more hair in the brush and the shower. Diffuse, with no bald patches. |
| Shedding peak | Month 3–6 | Heaviest shedding, the whole head affected. Pull test clearly positive. |
| Easing off | Month 6–9 | Shedding drops noticeably. Weight stabilizes and improved nutrition takes effect. |
| Regrowth | Month 6–12 | New fine hairs visible at the hairline and part. Density slowly increases. |
| Cosmetic recovery | Month 12–18 | Hair density approaches its starting level. With pure TE, full recovery is realistic. |
If the weight loss continues, for example through further dose increases, the shedding phase can drag on beyond 6 months. Full cosmetic recovery then only sets in once your weight has stabilized. One important exception: with an unmasked, genetically driven AGA, full regrowth on its own is not to be expected.
Who is most at risk?
Not everyone loses hair on semaglutide. Your risk depends on several specific factors.
- The extent of the weight loss. The single strongest predictor. Losing more than 20% of body weight means a 5.3% alopecia rate versus 2.5% in those losing less than 20%. Around a third of Wegovy patients lose more than 20%.
- Dose and speed of titration. Wegovy (2.4 mg) shows the signal, Ozempic (max. 2.0 mg) does not. Rapid dose jumps without plateau phases speed up the weight loss and with it the risk.
- Female sex. In the Wegovy label, 4% of women are affected versus 0.9% of men. In a Canadian study the adjusted hazard ratio for women was 2.08, while no significant signal was found in men.
- Pre-existing nutrient deficiencies. Anyone who already has low ferritin or zinc, or a marginal protein intake, before starting treatment is more vulnerable.
- A genetic predisposition to AGA. Sons of bald fathers carry a 5 to 6 times higher AGA risk. More than 90% of those affected in one review had a personal history of hair loss.
So the most important difference lies in the indication: obesity patients on Wegovy lose weight more aggressively and are affected more often, while diabetes patients on Ozempic or Rybelsus are affected far less. If you want to know whether your own predisposition plays a part, a professional assessment of your hair status helps before you start worrying.
What exactly is semaglutide? Brands and indications
Semaglutide is the active substance behind three well-known brands from the manufacturer Novo Nordisk. All three contain the same substance, but differ in how they are taken, the dose and the approved indication.
- Ozempic (subcutaneous, 0.5 to 2.0 mg per week): approved for type 2 diabetes and cardiovascular risk reduction, FDA approval in 2017. You will find brand-specific detail on hair loss on our dedicated Ozempic page.
- Wegovy (subcutaneous, 2.4 mg per week): approved for chronic weight management in obesity, FDA approval in 2021. This is the one that lists hair loss in its label. We cover Wegovy in depth in a separate article.
- Rybelsus (oral, 7 to 14 mg daily): approved for type 2 diabetes, FDA approval in 2019. The first orally available GLP-1 RA.
The mode of action of all three: stimulation of glucose-dependent insulin secretion, inhibition of glucagon release, slowed gastric emptying and central appetite control. The strong effect on weight loss (−14.9% on Wegovy over 68 weeks) is at the same time the reason for the raised hair-loss risk compared with the diabetes products.
Semaglutide and hereditary hair loss: the unmasking problem
Here is the point at which a temporary problem can turn permanent. In people with a genetic predisposition, the rapid weight loss can uncover or accelerate an androgenetic alopecia that had until then been invisible. The mechanism: in fatty tissue, estrogen is produced via the enzyme aromatase. When the body-fat percentage falls quickly, the balance shifts in favor of the androgens. This relative androgen excess encourages the DHT-driven miniaturization of follicles in genetically susceptible people.
The data back this up. In the TriNetX cohort the AGA signal appeared as early as 6 months (aOR 1.62) and remained stable at 12 months (aOR 1.64). This early and stable AGA association points to unmasking rather than just a temporary effluvium. The crucial difference for you: a pure telogen effluvium recovers on its own within 6 to 12 months. An unmasked AGA carries on progressing without treatment, even if you stop semaglutide.
Signs that it is an AGA and not just a TE: a patterned rather than diffuse loss, a positive family history, no full recovery after 12 months, and an increasingly sparse area at the temples or crown. Where your own status sits on the Hamilton-Norwood scale is best determined by a professional.
Diffuse or patterned? This decides what to do
Diffuse telogen effluvium (reversible). If the loss is even across the whole scalp, you do not need a hair transplant. Here what helps is patience (6 to 12 months), enough protein, a checked ferritin level and a moderate pace of weight loss. The hair comes back on its own.
Unmasked hereditary alopecia (permanent). If the weight loss uncovers an AGA that was already present, meaning a receding hairline, a thinning crown or a clear pattern, it will not recover on its own. That is exactly when a permanent solution becomes the topic. A professional hair analysis reliably establishes which of the two you are dealing with, before you change anything about your treatment.
What can I do about hair loss on semaglutide?
You can actively counter it, above all through your diet. The strongest modifiable lever is your protein intake.
- Prioritize protein. Aim for 1.2 to 1.6 g per kg of body weight per day, spread across 3 to 4 meals of 25 to 30 g each. With a dampened appetite, this is the most important conscious step you can take.
- Check your micronutrients. Raise ferritin above 40 ng/mL, ideally above 70 ng/mL. Supplement zinc and vitamin D only where a deficiency is confirmed. Have your thyroid level (TSH) checked.
- Titrate slowly. Where possible, keep your weight loss to 0.5 to 1.0 kg per week. If hair loss is heavy, pause the dose increase and optimize your nutritional status first.
- Gentle hair care. Cut back on heat styling, use soft brushes, and avoid the pull of tight braids.
Does hair grow back after semaglutide?
If the hair loss continues despite better nutrition, there are proven options. The causal measures, that is topping up ferritin and protein, take priority over symptomatic treatments.
- Topical minoxidil 5%. It lengthens the anagen phase and improves blood flow at the follicle. In an open-label study in telogen effluvium, hair density improved markedly.
- Oral low-dose minoxidil. Off-label, and only under medical supervision. In studies more than 50% of users showed an improvement. Because of possible cardiovascular side effects such as low blood pressure, palpitations or fluid retention, it absolutely belongs in a doctor’s hands.
- Correct nutrient deficiencies. The most important and root-cause measure.
- PRP (platelet-rich plasma therapy). Available at Elithair as an add-on, with good evidence above all for AGA.
If AGA is suspected, a diagnosis by a dermatologist is decisive, because prescription-only drugs such as finasteride or spironolactone can only be prescribed by a doctor. With a persistent loss of more than 6 months and no improvement, trichoscopy is worthwhile, that is the microscopic examination of the scalp and hair roots.
The Elithair approach: when does a hair transplant make sense?
A clear statement first: for a pure telogen effluvium after semaglutide, a hair transplant is neither needed nor sensible. The follicles are intact and only temporarily at rest. Once your weight stabilizes and your nutrient supply is right, the loss corrects itself within 6 to 18 months. A transplant would change nothing about the underlying cause.
A transplant only becomes relevant in a different scenario: when semaglutide has unmasked a genetically driven AGA. This one progresses and does not recover on its own. If after 12 months you see no full regrowth, a typical AGA pattern becomes visible and the donor area is stable, a transplant can be a permanent solution. The prerequisite is always a clean diagnosis of whether you have TE, AGA or a mixed form.
Semaglutide compared with other GLP-1 drugs
Semaglutide is not the only drug in this class. The second big player is tirzepatide, a dual GIP/GLP-1 receptor agonist found in the brands Mounjaro and Zepbound. The table below ranks the hair-loss risk by the decisive factor, the weight loss.
| Product | Active substance | Alopecia in label | Incidence | Weight loss |
|---|---|---|---|---|
| Wegovy | Semaglutide | Yes | 3.3% (vs. 1.0%) | −14.9% (68 wks) |
| Ozempic | Semaglutide | No (post-marketing only) | not quantified | −3 to 6 kg (diabetes) |
| Rybelsus | Semaglutide (oral) | No | not quantified | −4 kg (diabetes) |
| Zepbound | Tirzepatide | Yes | ~5% (women 7.1%) | −22.5% (72 wks) |
| Mounjaro | Tirzepatide | Yes (post-marketing) | ~5.7% | −11 kg (diabetes) |
| Liraglutide | Liraglutide | No | no signal | −5 to 8% |
The pattern is unmistakable. The hair-loss signal appears with the weekly drugs that produce strong weight loss, namely semaglutide (Wegovy) and tirzepatide (Zepbound, Mounjaro). Daily drugs with smaller weight loss, such as liraglutide, show no significant signal. Tirzepatide achieves more weight loss on average (−22.5% versus −14.9%) and accordingly has slightly higher alopecia rates in the clinic. Whether the additional GIP receptor plays a part of its own here is not proven. The primary driver remains the extent and pace of the weight loss, not the molecular structure.
In our clinics we are increasingly seeing patients who lose hair on weight-loss shots and panic. In the vast majority of cases it is a temporary telogen effluvium that recovers on its own. The real question is not whether to stop semaglutide, but whether a hereditary alopecia has been unmasked in the background. That can only be reliably established with a professional hair analysis.
Dr. Balwi, Medical Director at Elithair
When should you see a doctor? The warning signs
A diffuse, slowly easing thinning is usually harmless. But with these signs you should seek medical advice promptly:
- Patchy hair loss with round, well-defined bald spots. Suspicious of alopecia areata, where early treatment matters.
- Redness, itching, pain, pustules or crusting of the scalp. A possible sign of scarring alopecia, which risks irreversible follicle loss.
- Very rapid, massive loss of more than 300 hairs a day within weeks. Other causes such as thyroid or autoimmune disease should be ruled out.
- Loss lasting more than 6 months with no improvement despite better nutrition, or no regrowth after 12 months.
- Patterned loss with a positive family history. Suspicious of an unmasked AGA.
Frequently asked questions about semaglutide and hair loss
The verdict: does semaglutide cause hair loss?
Yes, semaglutide can trigger hair loss, but almost always only indirectly. The drug does not harm the hair follicles directly. Through a rapid weight loss it leads to a telogen effluvium, which as a rule is reversible. Wegovy, because of its higher dose and the more dramatic weight loss, is affected more often than Ozempic or Rybelsus. Anyone who keeps an eye on their protein intake, tops up their iron stores and loses weight at a moderate pace can reduce the loss considerably. It only gets tricky when a hereditary alopecia is unmasked, because that does not recover on its own. When in doubt, the view of a specialist clinic is worth having before you change anything about your treatment.
Sources
- Novo Nordisk. Wegovy (semaglutide) Prescribing Information. FDA, 2026. accessdata.fda.gov
- Novo Nordisk. Ozempic (semaglutide) Prescribing Information. FDA, 2025. accessdata.fda.gov
- Novo Nordisk. Wegovy Summary of Product Characteristics (SmPC). UK EMC, 2024. medicines.org.uk
- Wilding JPH et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1). N Engl J Med. 2021. NEJM
- Garvey WT et al. Two-year effects of semaglutide (STEP 5). Nat Med. 2022. PMC
- Godfrey H et al. Alopecia associated with semaglutide and tirzepatide: a FAERS pharmacovigilance study. JEADV. 2025. PubMed
- Vidal SI, Akiska YM et al. Increased risk of hair loss with GLP-1 receptor agonists: TriNetX cohort study. JAAD Int. 2026. PMC
- Burke JM et al. GLP-1 receptor agonist medications and hair loss: a retrospective cohort study. J Am Acad Dermatol. 2025. JAAD
- Gupta AK et al. GLP-1 therapies and hair loss: a systematic review. Science Progress. 2026. Sage
- Rojas Lopez RF et al. Alopecia as an emerging adverse effect of GLP-1 receptor agonists: a scoping review. Cureus. 2025. PMC
- Alsuwailem OA et al. Hair loss associated with GLP-1 receptor agonist use: a systematic review. Cureus. 2025. PMC
- Haykal D. Alopecia and Semaglutide: Connecting the Dots for Patient Safety. J Cosmet Dermatol. 2025. PMC
- Alzahrani WS et al. Alopecia areata following semaglutide treatment: a case report. JAAD Case Rep. 2025. PMC
- Sodhi M, Etminan M et al. Risk of Hair Loss with Semaglutide for Weight Loss. medRxiv Preprint. 2025. medRxiv
- StatPearls. Telogen Effluvium. NIH/NCBI Bookshelf. 2024. NCBI
- StatPearls. Androgenetic Alopecia. NIH/NCBI Bookshelf. 2024. NCBI
- American Academy of Dermatology. How can GLP-1 drugs affect my skin, hair, and nails? 2026. aad.org
This article is for information only and does not replace medical advice. If your hair loss persists, or before making any changes to your medication, you should obtain a professional diagnosis and consult the doctor treating you.
{“@context”:”https://schema.org”,”@type”:”FAQPage”,”mainEntity”:[{“@type”:”Question”,”name”:”Does semaglutide cause hair loss?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”Yes, hair loss can occur. In the approval trials for Wegovy (semaglutide 2.4 mg) around 3% of patients were affected, compared with 1% on placebo. The cause is not a direct toxic effect of the drug, but predominantly a telogen effluvium following the rapid weight loss.”}},{“@type”:”Question”,”name”:”Is the hair loss on semaglutide reversible?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”In most cases, yes. A telogen effluvium is self-limiting: once your weight stabilizes and any nutrient deficiencies are corrected, the hair usually grows back within 6 to 12 months. If, however, a genetically driven AGA has been unmasked, full recovery is not to be expected without treatment.”}},{“@type”:”Question”,”name”:”How can I stop the hair loss on semaglutide?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”The most important steps: enough protein (at least 1.2 g/kg/day), check ferritin and iron, supplement zinc and vitamin D only where there is a deficiency, and slow the weight loss where you can. With persistent loss, topical minoxidil may help in consultation with your doctor.”}},{“@type”:”Question”,”name”:”What kind of hair loss does semaglutide cause?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”Primarily a telogen effluvium, that is a diffuse thinning across the whole scalp, 2 to 4 months after starting treatment. In a cohort of 283 users, however, androgenetic alopecia was the most commonly diagnosed subtype, because semaglutide can unmask a genetic predisposition.”}},{“@type”:”Question”,”name”:”When does the hair loss on semaglutide start?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”As a rule, 2 to 4 months after starting treatment or after a significant dose increase. This delay matches the normal duration of the telogen phase of around 2 to 3 months. The heaviest shedding is usually between month 3 and 6.”}},{“@type”:”Question”,”name”:”Is the hair loss worse on higher doses of semaglutide?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”Yes. The risk correlates with the extent of the weight loss. With more than 20% body-weight loss, the alopecia rate was 5.3% versus 2.5% in those losing less than 20%. Wegovy (2.4 mg) leads to greater weight loss than Ozempic and therefore shows the hair-loss signal in its label, while Ozempic does not.”}},{“@type”:”Question”,”name”:”Do women lose hair on semaglutide more often than men?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”Yes, markedly. In the Wegovy label, 4% of women are affected versus 0.9% of men. In one study the adjusted hazard ratio for women was 2.08, while no significant signal was found in men. Women generally have a higher predisposition to telogen effluvium and to female-pattern hair loss.”}},{“@type”:”Question”,”name”:”Should I stop semaglutide because of hair loss?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”Hair loss alone is not a medical reason to stop semaglutide. The telogen effluvium usually recovers even while you stay on treatment, once your weight stabilizes. The benefit in obesity and diabetes outweighs it. Stopping abruptly can also bring back weight gain, which in turn means renewed stress for your hair. Always discuss any dose adjustment with the doctor who prescribed it.”}},{“@type”:”Question”,”name”:”Does Ozempic cause as much hair loss as Wegovy?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”No. Ozempic (diabetes, max. 2.0 mg) leads to far less weight loss than Wegovy (obesity, 2.4 mg) and is not listed as an alopecia risk in the FDA label. Both contain the same active substance, semaglutide, but the slower pace of weight loss on Ozempic triggers a telogen effluvium less often.”}},{“@type”:”Question”,”name”:”Which supplements help with semaglutide hair loss?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”Only supplements for a confirmed deficiency make sense: iron or ferritin, zinc and vitamin D. Biotin has no proven benefit in people who are well supplied, and at high doses it can distort lab values. A complete multivitamin is harmless, but it does not replace the targeted topping-up of genuine deficiencies.”}},{“@type”:”Question”,”name”:”Do I need a hair transplant if I lose hair on semaglutide?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”With a pure telogen effluvium, no, because the follicles are intact and the loss is temporary. A transplant can only become sensible once semaglutide has unmasked a hereditary AGA that progresses without treatment. A hair analysis establishes which case applies.”}},{“@type”:”Question”,”name”:”How long does the hair loss on semaglutide last?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”The shedding phase typically begins 2 to 4 months after starting treatment and lasts around 3 to 6 months. Full cosmetic recovery takes about 12 to 18 months. With sustained heavy weight loss, the loss can last longer until your weight stabilizes.”}}]} { “@context”: “https://schema.org”, “@type”: “MedicalWebPage”, “name”: “Semaglutide and Hair Loss: Does the Drug Cause Hair Loss and Is It Reversible?”, “url”: “https://elithair.com/blog/semaglutide-hair-loss/”, “lastReviewed”: “2026-06-05”, “reviewedBy”: { “@type”: “Person”, “name”: “Dr. Imad Moustafa”, “jobTitle”: “Hair Transplant Physician”, “image”: “https://elithair.com/de/wp-content/uploads/sites/2/2026/05/dr-moustafa.webp”, “worksFor”: { “@type”: “MedicalOrganization”, “name”: “Elithair” } }, “author”: { “@type”: “Organization”, “name”: “Elithair” }, “about”: { “@type”: “MedicalCondition”, “name”: “Telogen Effluvium” } }
Dr. Imad Moustafa
Hair transplant specialist