
You have been injecting Ozempic for a few months, your blood sugar is finally under control, and suddenly there are more hairs on your pillow each morning than there used to be. Clumps catch in the brush, your ponytail feels thinner, your part looks wider. The obvious suspicion: is it the medication? Plenty of Ozempic users share this worry, and it does not come out of nowhere. In 2024 the FDA formally reviewed reported cases of hair loss linked to semaglutide, and the reports are piling up in online forums.
The answer is more nuanced than the headlines suggest. Yes, hair loss can occur while you are on Ozempic. No, the drug does not attack your hair follicles directly. What actually happens, in the vast majority of cases, is telogen effluvium: a temporary, diffuse hair loss triggered by rapid weight loss and nutrient deficiencies. We unpack exactly that mechanism here, along with the figures from the clinical trials and what you can do about it.
In short: does Ozempic cause hair loss?
Yes, hair loss can occur while you are on Ozempic, but not through direct damage to the hair root. The usual trigger is telogen effluvium: a temporary, diffuse shedding caused by rapid weight loss and the nutrient deficiencies that come with it. In the vast majority of cases it is fully reversible.
- Cause: the weight loss and nutrient deficiencies, not any drug toxicity from semaglutide.
- Temporary and reversible: regrowth usually begins 6 to 9 months after your weight stabilizes, with full recovery in 12 to 18 months.
- Label difference: hair loss is not listed as a common side effect on the Ozempic FDA label, whereas it is for Wegovy (same active ingredient, higher dose) at 3% versus 1% on placebo.
- When to see a doctor: with patchy loss, scarring, or if nothing regrows after 12 months (a sign of hereditary hair loss).
So if you are losing hair right now, Ozempic is rarely the sole culprit. The rapid weight loss is usually behind it, and sometimes a previously hidden hereditary predisposition. If in doubt, have your hair assessed by a professional before you stop your medication in a panic. For a deeper look at the active ingredient itself, see our hub article on semaglutide and hair loss.
Summary
- The key facts at a glance
- Does Ozempic cause hair loss? The clinical evidence
- How does hair loss on Ozempic present?
- Why does it happen? The mechanism behind the hair loss
- The timeline: when does the hair loss start, and when does it grow back?
- Who is most at risk?
- What exactly is Ozempic?
- Ozempic and hereditary hair loss: the unmasking
- Prevention: how to guard against hair loss while losing weight
- Treatment and regrowth: what actually helps
- The Elithair approach: when does a hair transplant make sense?
- Ozempic compared with other GLP-1 medications
- When you should see a doctor: the warning signs
- Frequently asked questions about Ozempic and hair loss
- Conclusion: does Ozempic cause hair loss?
- Sources
The key facts at a glance
- Incidence in trials: the SUSTAIN diabetes trials of Ozempic (up to 2 mg) recorded no meaningful hair-loss signal. On Wegovy (2.4 mg, obesity), hair loss occurred in 3% of patients versus 1% on placebo.
- Real-world estimate: according to Dr. Kathy Zhou of the Cleveland Clinic, around 25% to 33% of Ozempic users experience some degree of hair thinning in clinical practice.
- Reversible: yes, usually completely. Spontaneous recovery within 6 to 12 months once your weight stabilizes.
- Timeline: onset typically 2 to 4 months after starting treatment or increasing the dose, peaking around month 4 to 6, with regrowth from month 6 to 9.
- Main risk factor: rapid weight loss. With more than 20% body-weight loss on semaglutide, the alopecia rate rose to 5.3%.
- No direct follicle damage: there is no evidence that semaglutide damages the hair root directly.
Does Ozempic cause hair loss? The clinical evidence
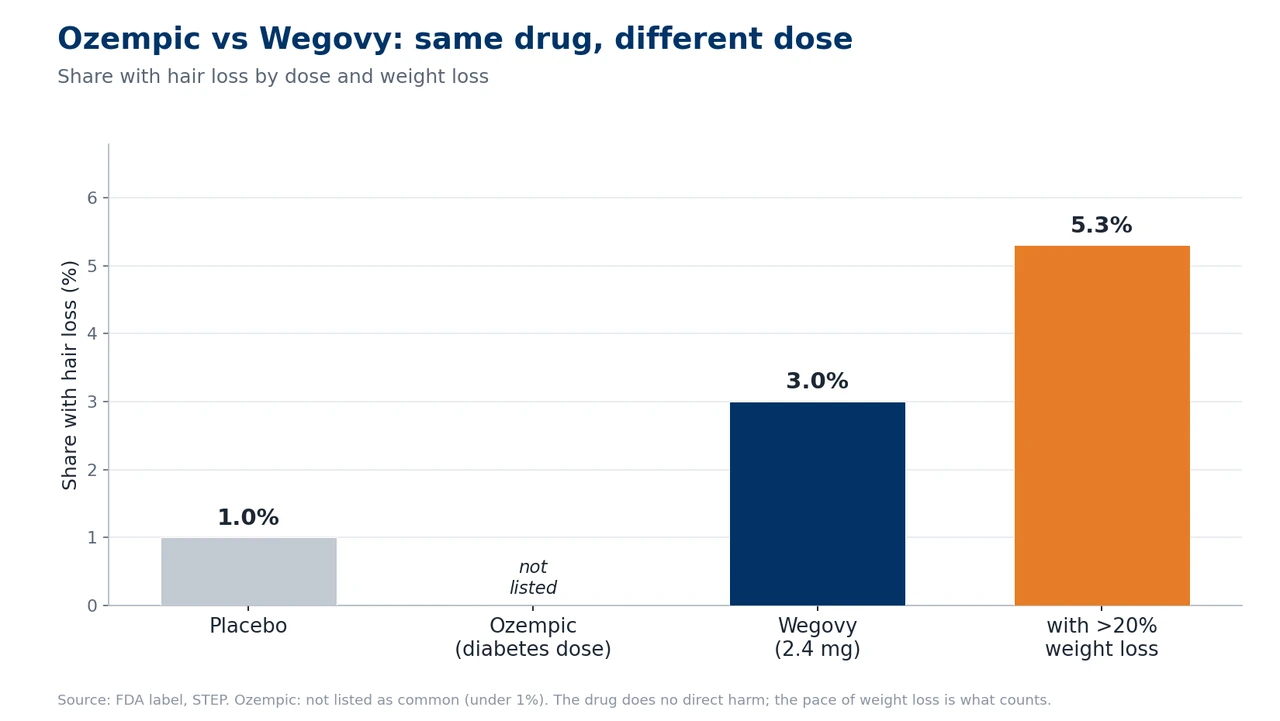
The crucial point most reports miss: Ozempic and Wegovy contain the same active ingredient, semaglutide, yet they are treated differently on the FDA label. For Ozempic (maximum dose 2 mg per week, approved for type 2 diabetes), alopecia is not listed as a common side effect in section 6.1 of the Prescribing Information. In the SUSTAIN trials, the mean weight loss was only around 3 to 6 kg, too little to trigger a meaningful telogen effluvium.
With Wegovy it is a different story. Here hair loss is explicitly listed: 3% in adults versus 1% on placebo. The FDA’s wording, in essence, is that the hair-loss reactions on Wegovy were associated with the weight reduction. The difference therefore comes down purely to dose and weight loss: Wegovy (2.4 mg) produced a mean weight loss of 14.9% in the STEP 1 trial, enough for a telogen effluvium. You can read more about how the two brands compare in our article on Wegovy and hair loss.
The SUSTAIN program: why Ozempic stays clean on the label
Ozempic’s FDA approval rests on the SUSTAIN trial program. In SUSTAIN 6, a cardiovascular safety trial of 3,297 people with type 2 diabetes over 104 weeks, the mean weight loss on 1 mg was only 3.6 kg. No significant alopecia signal emerged. SUSTAIN 7, with around 6.5 kg of weight loss, likewise reported no hair-loss signal. The limited weight loss at therapeutic diabetes doses neatly explains why the label carries no alopecia here.
FAERS and the 2024 FDA review
The FAERS pharmacovigilance database recorded around 199 reports of alopecia on semaglutide for 2022 and 2023. In January 2024 the FDA reviewed whether regulatory action might be needed, without establishing definitive causation. A FAERS analysis by Godfrey and colleagues (JEADV, 2025) calculated a reporting odds ratio of 2.46 for semaglutide. One important caveat: FAERS does not separate by formulation, so the data aggregate Ozempic and Wegovy reports together.
What the large cohort studies show
More telling than individual reports are the large database analyses. A multicenter TriNetX cohort study (Vidal, Akiska et al., JAAD International 2026) of 547,993 matched adults found, at 12 months, an increased risk of telogen effluvium (adjusted odds ratio 1.76) and of androgenetic alopecia (aOR 1.64). A systematic review by Gupta and colleagues (Science Progress 2026) calculated a 3.4-fold increased risk of alopecia in GLP-1 users versus placebo in its meta-analysis, with a confirmed dose dependency for semaglutide.
One important point comes through consistently across all these reviews: there is no definitive proof of causation showing that the active ingredient semaglutide itself causes hair loss. The most likely mechanism remains a secondary telogen effluvium driven by the stress of weight loss.
How does hair loss on Ozempic present?
The typical pattern is a diffuse telogen effluvium: the hair thins evenly across the whole scalp, without isolated bald patches forming. You notice markedly more hair in the brush, in the drain and on the pillow. Where 50 to 100 hairs would normally fall out per day, with telogen effluvium it can be 200 to 300 or more. In women, a widening part is often the first thing to become visible.
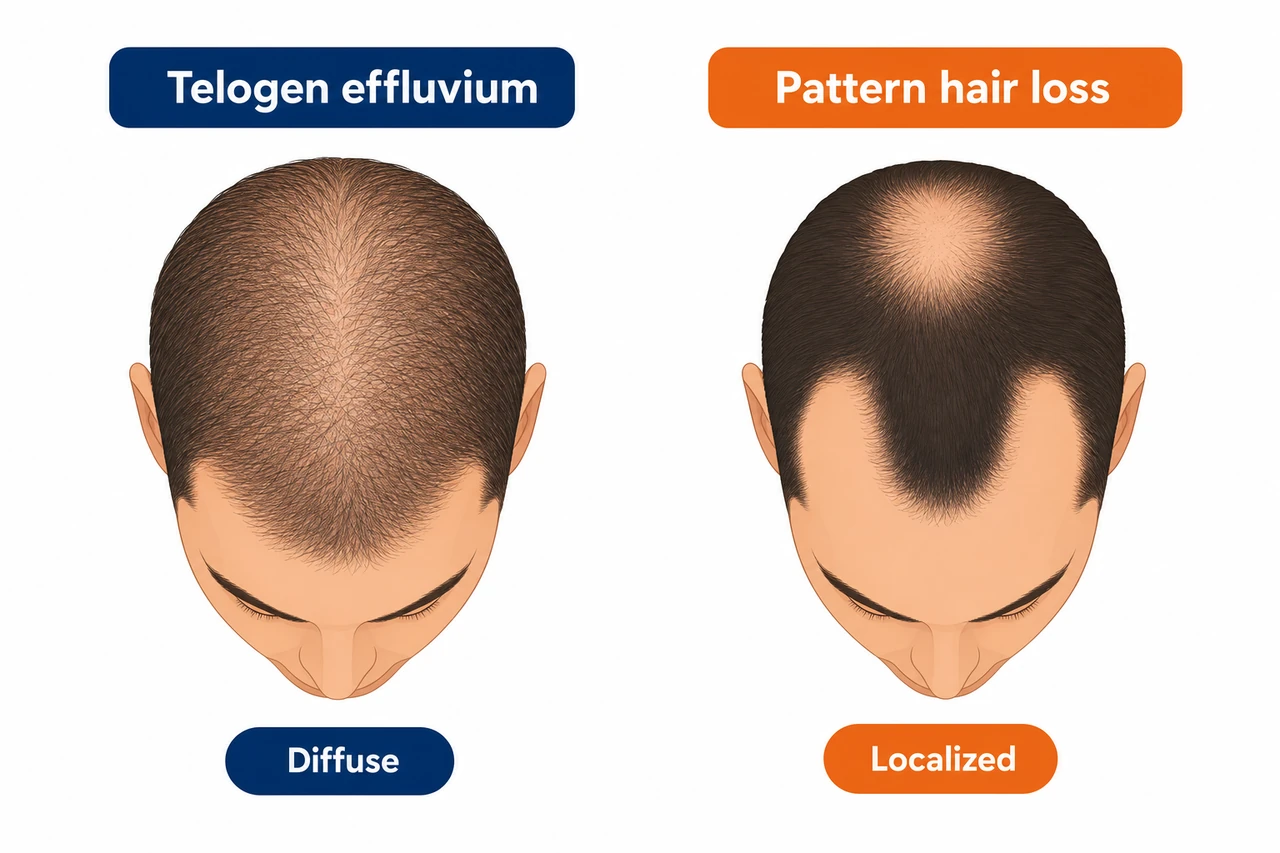
The distinction from androgenetic alopecia, the hereditary form of hair loss, is important. That follows a pattern: in men, receding temples and thinning at the crown along the Norwood-Hamilton scale, and in women, thinning at the part. It involves follicular miniaturization, and without treatment the loss is permanent. A third, rare form is alopecia areata, with round, sharply defined bald patches. It has been described in a case report following semaglutide use and belongs in a dermatologist’s hands. For how the natural hair cycle works in the first place, see our overview of the hair growth cycle.
Why does it happen? The mechanism behind the hair loss
The main mechanism is called telogen effluvium, triggered by rapid weight loss. Under heavy calorie restriction the body switches into a conservation mode and redirects energy and nutrients away from non-essential functions such as hair growth and toward the vital organs. Dr. Zhou of the Cleveland Clinic puts it neatly: the body perceives the weight loss as stress and begins to reserve resources for the important organs. Many hair follicles then move prematurely out of the growth phase and into the resting phase. Under severe physiological stress, as many as 70% of actively growing hairs can be affected at once.
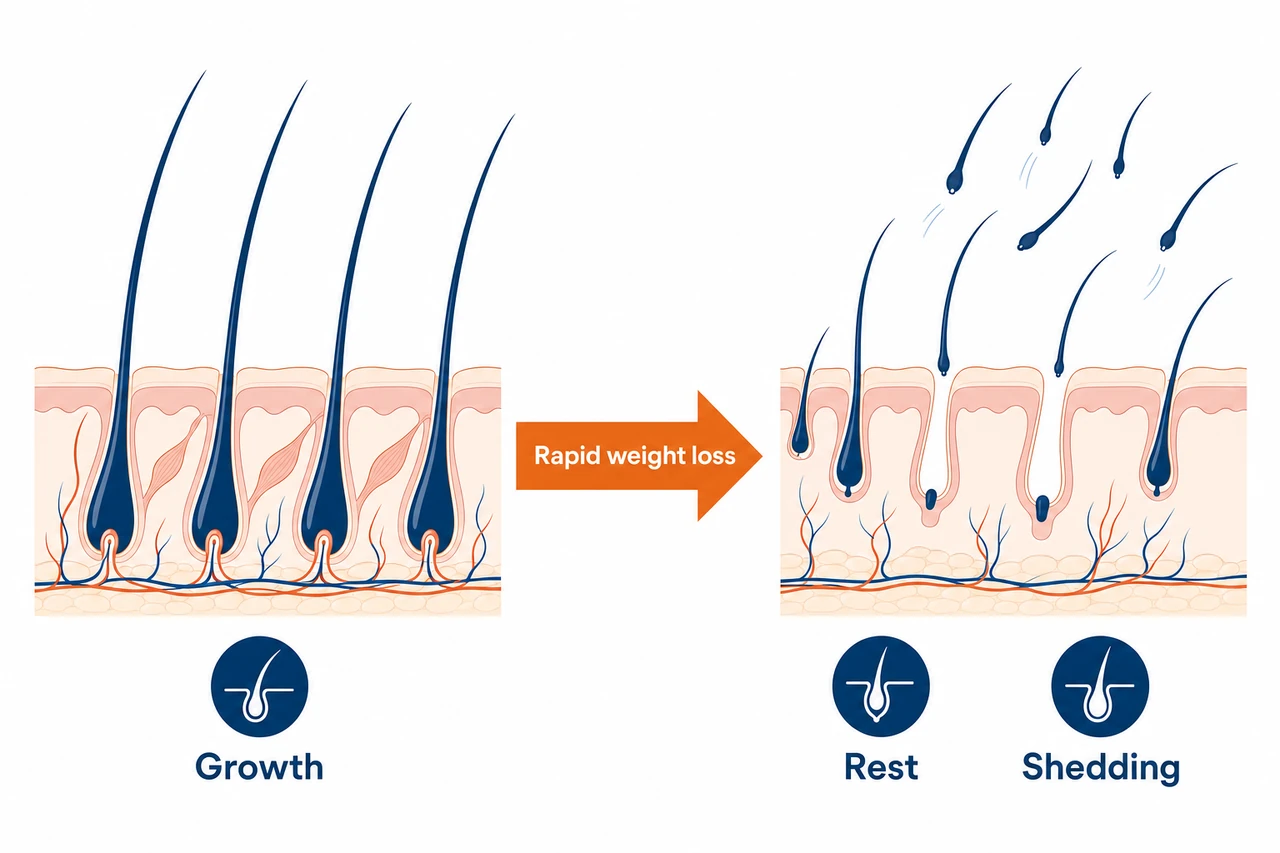
The strongest evidence for this mechanism is the correlation with the extent of weight loss: patients who lost more than 20% of their body weight on semaglutide showed an alopecia rate of 5.3%, compared with 2.5% in those who lost less than 20%. The faster and more drastic your weight loss, the higher the risk.
Which nutrient deficiencies make the hair loss worse?
Ozempic strongly suppresses appetite, and this is precisely where a hidden danger lies. Eating significantly less puts you at risk of running short on the very building blocks your hair needs:
- Protein: hair is around 90% keratin. With too little protein intake (below 0.8 g/kg/day), keratin synthesis stalls and the risk of telogen effluvium rises sharply.
- Iron and ferritin: iron is a cofactor for DNA synthesis in the hair matrix cells. For robust follicle growth, a target ferritin level above 70 ng/mL is recommended.
- Zinc: patients with telogen effluvium show significantly lower zinc levels. Zinc is essential for cell division in the hair root.
- Vitamin D: in one study of GLP-1 users with hair loss, 98.6% had insufficient vitamin D levels.
There is also a hormonal component: calorie restriction activates the stress axis, and raised cortisol levels can push hair follicles further into the resting phase. The psychological strain of the hair loss itself plays its part too, and can amplify the telogen effluvium in a vicious circle. What is clear, though, is this: there is no proven direct follicle-toxic effect of the active ingredient semaglutide. GLP-1 receptors have been detected in mouse hair follicles, but a functional expression in human follicles has not yet been confirmed.
The timeline: when does the hair loss start, and when does it grow back?
Telogen effluvium follows a characteristic timeline, and that helps you make sense of your own course. The hair loss does not start right away, but with a typical delay after the triggering stress.
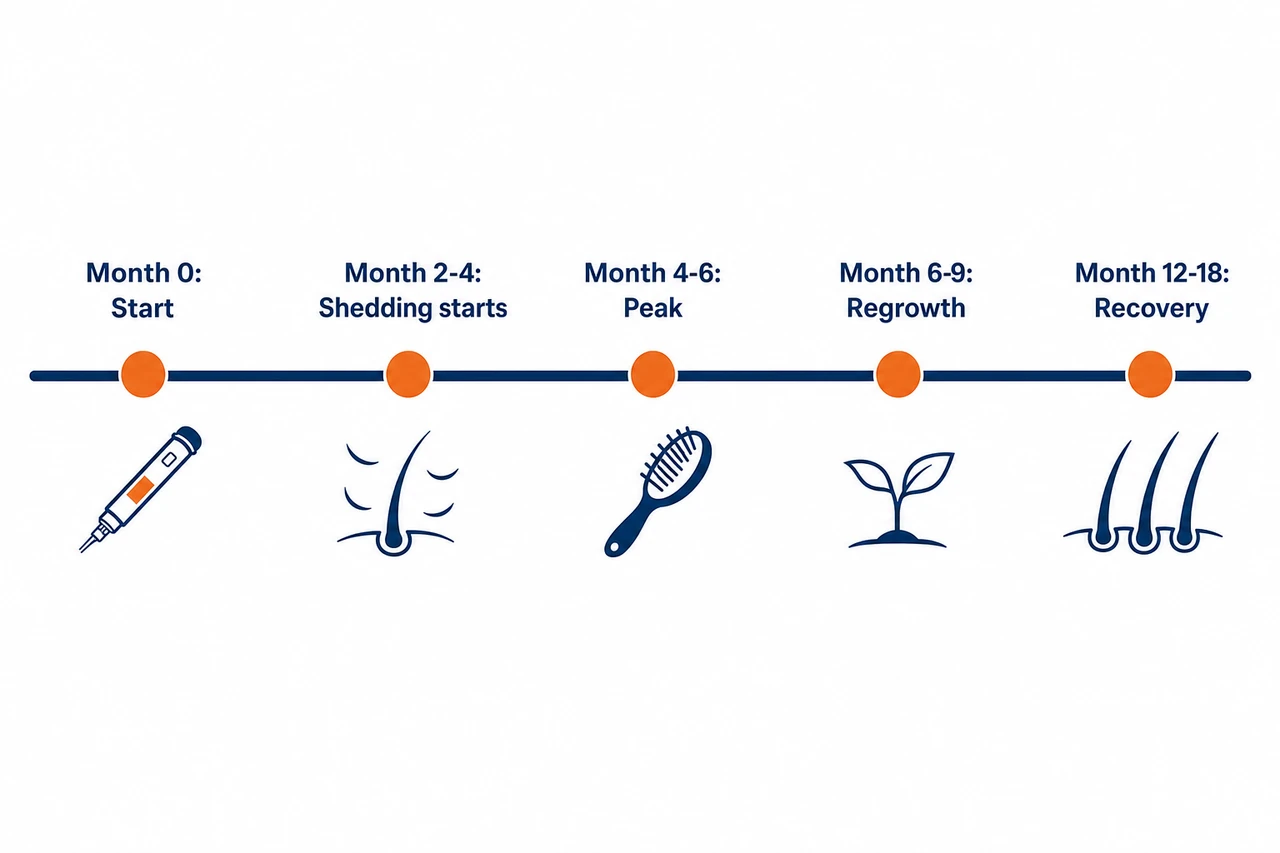
- Onset: 2 to 4 months after starting treatment or after a marked dose increase (for example from 0.5 mg to 1 mg). Sometimes a latency of up to 6 months.
- Peak: around month 4 to 6, the heaviest shedding phase with clumps in the brush.
- Plateau: after 3 to 6 months of active shedding, things stabilize once your weight settles and your nutrient status improves.
- Regrowth: visible from month 6 to 9 after your weight stabilizes, with full cosmetic recovery in 12 to 18 months.
A difference from Wegovy shows up here too: in the diabetes indication, with a moderate weight loss of 3% to 7%, the shedding phase on Ozempic is shorter and less pronounced. Anyone using Ozempic off-label for aggressive weight loss, on the other hand, edges closer to the Wegovy risk level. With sustained rapid weight loss and no plateau, the telogen effluvium can even become chronic, lasting longer than 6 months.
Who is most at risk?
Not every Ozempic user loses hair, and the risk is by no means spread evenly. These factors determine how likely telogen effluvium is for you:
- Extent and pace of weight loss: losing more than 20% of your body weight doubles the alopecia rate. A loss of more than 1 kg per week marks a clearly elevated risk.
- Off-label rather than diabetes: the diabetes indication, with moderate weight loss, carries a much lower risk than off-label use for aggressive weight loss. The American Hair Loss Association explicitly warns of significant and potentially permanent hair loss when Ozempic is misused for rapid weight reduction.
- Sex: women are disproportionately affected. In an analysis by researchers at the University of British Columbia (Sodhi et al.), the adjusted hazard ratio for women was 2.08. Across analyses, 63% to 78.6% of those affected were women.
- Pre-existing deficiencies: iron deficiency, zinc deficiency or a vitamin D shortfall before starting treatment all raise the risk.
- Genetic predisposition: anyone with a family tendency to hereditary hair loss risks a permanent worsening rather than a merely temporary loss.
- PCOS and a hormonal predisposition: women with polycystic ovary syndrome, who often use Ozempic off-label for weight loss, frequently already have some androgenetic thinning. The weight-related hair loss can additionally unmask that predisposition.
What exactly is Ozempic?
Ozempic is Novo Nordisk’s brand name for the active ingredient semaglutide, a GLP-1 receptor agonist. The FDA approved Ozempic in December 2017 for blood-sugar control in adults with type 2 diabetes, and since 2020 additionally for reducing cardiovascular events in at-risk patients. Note: weight management is not an approved indication for Ozempic. For that there is Wegovy, which contains the same active ingredient at a higher dose.
Semaglutide works by binding to GLP-1 receptors, stimulating glucose-dependent insulin release, slowing gastric emptying and producing a feeling of fullness via the brain. The dose is increased slowly: four weeks at 0.25 mg as the starting dose, then 0.5 mg, and if needed up to 1 mg and a maximum of 2 mg, after at least four weeks at each step. The crucial difference from Wegovy lies in the maximum dose and the indication. Wegovy leads to around 15% weight loss, Ozempic to roughly 3% to 7%. That very difference explains the differing hair-loss risk profile.
Ozempic and hereditary hair loss: the unmasking
This is the trickiest part of the whole story. In people with a genetic predisposition, the weight loss from Ozempic can make a previously hidden androgenetic alopecia visible. While hair density was still high, the early hereditary thinning was barely noticeable. Once the telogen effluvium reduces overall density, the underlying pattern suddenly becomes obvious. Specialists call this unmasking.
On top of that, hormonal shifts during weight loss can accelerate the androgenetic follicular miniaturization. The TriNetX study found an increased androgenetic alopecia rate (aOR 1.64) at 12 months on GLP-1 therapy. The difference from telogen effluvium is decisive for your prognosis:
| Feature | Telogen effluvium after Ozempic | Androgenetic alopecia (unmasked) |
|---|---|---|
| Pattern | Diffuse, across the whole scalp | Patterned (temples, part) |
| Follicular miniaturization | No | Yes |
| Reversibility | Yes, spontaneous | No, chronically progressive |
| Time frame | Acute, 3 to 12 months | Slow, years to decades |
| Treatment | Optimize nutrients, minoxidil if needed | Minoxidil, finasteride, hair transplant |
The practical upshot: anyone with persistent, patterned hair loss beyond the expected telogen-effluvium window of 6 to 12 months may have a previously hidden androgenetic alopecia. For how hormones govern the hair follicle, our article on the interplay of hormones and hair goes into more detail.
Which case applies to you?
Diffuse and temporary (telogen effluvium): you do not need a hair transplant here. The loss is reversible. Give your hair 6 to 12 months, make sure you get enough protein, have your ferritin checked, and clarify your status with a hair analysis if you are unsure.
Patterned and lasting (unmasked hereditary alopecia): if the weight loss exposes an underlying androgenetic alopecia (a receding hairline, a thinning crown, patterned thinning), the hair in these zones will not grow back on its own. This is a case for a permanent solution. A free hair analysis will show you which path is the right one.
Prevention: how to guard against hair loss while losing weight
The good news is that you can actively lower the risk. The single most important lever is protein intake. Because Ozempic curbs your appetite, many users unknowingly fall short of their needs. Aim for 1.2 to 1.6 g of protein per kilogram of body weight per day, spread across 3 to 4 meals of 25 to 30 g each. Protein shakes, lean meat, eggs, legumes and Greek yogurt all help you get there.
With micronutrients, the rule is: test, do not supplement blindly. Have your ferritin, zinc, vitamin D, B12 and TSH checked before starting treatment and then every three months. Supplement in a targeted way only where a deficiency is confirmed. A second lever is the pace: follow the intended slow titration and do not skip any dose steps. Dr. Zhou advises avoiding the “cliff effect”, where the weight drops too fast. Where possible, limit the loss to 0.5 to 1 kg per week.
Treatment and regrowth: what actually helps
If the hair loss is already under way, there are effective options. Correcting nutrient deficiencies always comes first: minoxidil on a deficient foundation works only to a limited degree. First optimize ferritin, zinc, protein and vitamin D, then treat in a targeted way.
- Topical minoxidil 5%: in an open-label study of telogen effluvium, hair density improved measurably. FDA-approved for androgenetic alopecia, used off-label for telogen effluvium.
- Oral minoxidil (off-label): in a multicenter study of 105 patients, 52.4% showed an improvement. It is prescription-only and, because of possible cardiovascular side effects (a drop in blood pressure, fluid retention, a racing heart), absolutely belongs in specialist hands, especially as many Ozempic users have a cardiovascular risk profile. A medical assessment before starting is essential.
- PRP (platelet-rich plasma): a meta-analysis of 21 studies showed significant improvements in hair density and thickness. A sensible adjunct option for persistent telogen effluvium.
- Dermatological assessment: a trichogram and dermoscopy clarify whether this is a pure telogen effluvium or whether there is an androgenetic component. Recommended for hair loss that persists beyond 6 months.
With the right nutrient therapy and a stable weight, visible regrowth can be expected within 6 to 9 months. Patience is part of it, because the hair cycle cannot be rushed.
The Elithair approach: when does a hair transplant make sense?
Here is the clear message first: with a pure telogen effluvium, a hair transplant is neither necessary nor sensible. Telogen effluvium is reversible, the follicles are intact and they recover on their own. As long as active shedding is going on, a transplant would even be counterproductive, because the transplanted hairs could shed in the same process.
A hair transplant only becomes relevant once a patterned hair loss persists after more than 12 months of weight stabilization and an optimized diet, and the diagnostics confirm an androgenetic alopecia. The most common candidate in this context is someone in whom Ozempic has exposed a previously latent hereditary predisposition. The transplant then treats the alopecia, not the telogen effluvium.
Many patients come to us anxious because they are losing hair on Ozempic or Wegovy. In most cases it is a temporary telogen effluvium caused by the weight loss, which resolves on its own. A transplant only comes into question once a hereditary alopecia shows itself after months of stabilization. The first and most important step is always an honest hair analysis.
Dr. Balwi, Medical Director at Elithair
If you want to know whether your telogen effluvium has settled or whether a permanent alopecia lies behind it, you can request a free hair analysis at Elithair. Our specialists assess the state of your hair and explain whether a conservative approach is enough or whether a hair transplant makes sense.
Ozempic compared with other GLP-1 medications
The hair-loss risk of the various GLP-1 drugs follows a simple logic: the more weight loss a medication produces, the higher the risk of telogen effluvium. The table below sets out the main products.
| Product | Active ingredient | Indication | Alopecia on FDA label? | Incidence (active drug) | Notable point |
|---|---|---|---|---|---|
| Ozempic (up to 2 mg) | Semaglutide | Type 2 diabetes | No, post-marketing only | Not captured in trials | Low risk at diabetes dose, higher off-label |
| Wegovy (2.4 mg) | Semaglutide | Obesity | Yes, section 6.1 | 3% (higher in women) | With more than 20% weight loss: 5.3% |
| Mounjaro (up to 15 mg) | Tirzepatide | Type 2 diabetes | Yes, post-marketing (2025) | around 5% (meta-analysis) | Dual GIP/GLP-1 receptor agonist |
| Zepbound (up to 15 mg) | Tirzepatide | Obesity | Yes, section 6.1 | around 5% (women 7.1%) | Largest sex-specific difference |
The most important comparison remains Ozempic versus Wegovy: the same active ingredient, with dose and indication alone explaining the different labeling. Tirzepatide, the active ingredient in Mounjaro and Zepbound, produces an even greater weight loss (up to 22.5% in SURMOUNT-1) and therefore a somewhat higher alopecia incidence. Whether the additional GIP-receptor effect acts independently on hair follicles is not proven. For the in-depth comparison of the active ingredients, see our hub articles on semaglutide and tirzepatide.
When you should see a doctor: the warning signs
An uncomplicated telogen effluvium settles on its own. Certain signs, however, should be assessed by a doctor promptly:
- Round, sharply defined bald patches: a possible sign of alopecia areata, an autoimmune process. Early treatment improves the prognosis.
- Redness, scaling, crusting or scarring of the scalp: a possible sign of scarring alopecia, which becomes irreversible if it is left too long.
- Very heavy hair loss with accompanying symptoms such as fatigue or cold intolerance: have your thyroid checked.
- Hair loss for more than 6 months with no improvement despite an optimized diet and a stable weight: a differential diagnosis is needed.
- No regrowth after 12 months: a sign of a latent androgenetic alopecia, dermatological assessment recommended.
One important note to close this section: do not stop Ozempic on your own because of hair loss. Stopping treatment carries real risks in type 2 diabetes, such as blood-sugar control spiraling out of control. Always discuss any change with the prescribing doctor.
Frequently asked questions about Ozempic and hair loss
Conclusion: does Ozempic cause hair loss?
Yes, hair loss can occur while you are on Ozempic, but it is almost never a direct drug effect. In the diabetes indication, with moderate weight loss, the risk is low, and alopecia does not appear as a common side effect on the FDA label. What you are seeing is usually a telogen effluvium caused by the rapid weight loss, temporary and reversible. With enough protein, a controlled pace and corrected nutrient deficiencies, you lower the risk considerably. If the loss persists beyond 12 months or shows a pattern, a previously hidden hereditary alopecia could be behind it. In that case a professional hair analysis is worthwhile before you decide on any further steps. For the complete overview of the active ingredient, see our article on semaglutide and hair loss.
Sources
- FDA Prescribing Information Ozempic (semaglutide), NDA 209637, Novo Nordisk, 2025. FDA
- FDA Prescribing Information Wegovy (semaglutide), NDA 215256, Novo Nordisk, 2024. FDA
- Wilding JPH et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1). N Engl J Med. 2021. NEJM
- Marso SP et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes (SUSTAIN 6). N Engl J Med. 2016. NEJM
- Godfrey H et al. Alopecia associated with semaglutide and tirzepatide: a FAERS disproportionality analysis. JEADV. 2025. PubMed
- Vidal SI, Akiska YM et al. Increased risk of hair loss with GLP-1 receptor agonists: a real-world TriNetX cohort study. JAAD International. 2026. PMC
- Gupta AK et al. GLP-1 therapies and hair loss: a systematic review. Science Progress. 2026. Sage
- Rojas Lopez RF et al. Alopecia as an Emerging Adverse Effect Associated With GLP-1 Receptor Agonists for Weight Loss: A Scoping Review. Cureus. 2025. PMC
- Alsuwailem OA et al. Hair Loss Associated With GLP-1 Receptor Agonist Use: A Systematic Review. Cureus. 2025. PMC
- Sodhi M et al. Risk of Hair Loss with Semaglutide for Weight Loss. medRxiv (Preprint). 2025. medRxiv
- Ohyama M et al. Topical minoxidil 5 % for telogen effluvium. J Dermatol. 2025. PMC
- Pugliese MT et al. Biotin supplementation for hair loss: systematic review. JCAD. 2024. PubMed
- Zhou K, MD (Cleveland Clinic). Can Ozempic Cause Hair Loss? Cleveland Clinic Health Essentials. 2025. Cleveland Clinic
- AAD. How can GLP-1 drugs affect my skin, hair, and nails? American Academy of Dermatology. 2026. AAD
- American Hair Loss Association. Guidance on hair loss associated with GLP-1 medications. 2025. AHLA
- StatPearls. Telogen Effluvium. NCBI Bookshelf. 2024. NCBI
This article is for information only and does not replace medical advice. Never stop a prescribed medication on your own. If your hair loss persists, you should seek a professional diagnosis.
{“@context”:”https://schema.org”,”@type”:”FAQPage”,”mainEntity”:[{“@type”:”Question”,”name”:”Does Ozempic cause hair loss?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”Ozempic (semaglutide) can trigger hair loss, but predominantly indirectly, through rapid weight loss and nutrient deficiencies, in other words as telogen effluvium. Unlike Wegovy, alopecia is not listed as a common side effect on the Ozempic FDA label, because diabetes doses produce smaller weight losses. In clinical practice, the Cleveland Clinic reports that 25% to 33% of users experience some form of hair thinning.”}},{“@type”:”Question”,”name”:”Why does Ozempic cause hair loss?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”Ozempic curbs your appetite and leads to rapid weight loss. The body reads the calorie deficit as stress and prioritizes nutrients for vital organs. Many hair follicles switch prematurely into the resting phase. About 2 to 4 months later these hairs shed in clumps, a classic telogen effluvium. Deficiencies in iron, zinc and protein make the effect worse.”}},{“@type”:”Question”,”name”:”Is hair loss from Ozempic permanent?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”In most cases, no. A pure telogen effluvium is fully reversible once your weight stabilizes and any nutrient deficiencies are corrected. Visible regrowth usually begins after 6 to 9 months. The loss can become permanent if Ozempic has unmasked a previously latent androgenetic alopecia. The American Hair Loss Association also warns of potentially permanent loss when the drug is misused for rapid weight loss.”}},{“@type”:”Question”,”name”:”How long does hair loss on Ozempic last?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”Active shedding begins 2 to 4 months after starting treatment, peaks around month 4 to 6, and tails off after a further 3 to 6 months, provided your weight stabilizes. Regrowth is visible from month 6 to 9, and full cosmetic recovery takes 12 to 18 months. Without a weight plateau, the shedding phase is prolonged accordingly.”}},{“@type”:”Question”,”name”:”How can I stop hair loss from Ozempic?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”The most effective measures: enough protein (1.2 to 1.6 g per kg of body weight daily), testing ferritin and zinc and supplementing in a targeted way where there is a deficiency, limiting weight loss to a maximum of 0.5 to 1 kg per week, and taking a daily multivitamin. For persistent loss, topical minoxidil 5% plus dermatological advice helps. Biotin is ineffective if you are adequately nourished.”}},{“@type”:”Question”,”name”:”Will my hair grow back after Ozempic hair loss?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”With a pure telogen effluvium, yes, completely. The follicles are intact and return to the growth phase once the stress is removed. The key factors are a stable weight, corrected nutrient deficiencies and enough protein. If an androgenetic alopecia has been unmasked, however, the hair in the affected zones does not come back fully, and medical advice is needed here.”}},{“@type”:”Question”,”name”:”Is hair loss a listed side effect of Ozempic?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”No, not in section 6.1 of the Prescribing Information (clinical-trials experience). For Wegovy, the same active ingredient at a higher dose for obesity, alopecia is explicitly listed (3% versus 1% placebo). For Ozempic, hair loss appears at most as a post-marketing report with no frequency given, because the SUSTAIN diabetes trials did not produce enough weight loss for a telogen effluvium.”}},{“@type”:”Question”,”name”:”Does Ozempic cause hair loss in women?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”Yes, women are disproportionately affected. In an analysis by researchers at the University of British Columbia (Sodhi et al.), the adjusted hazard ratio for hair loss in women on semaglutide was 2.08. Between 63% and 78.6% of all reported cases of GLP-1-associated alopecia were in women. Possible reasons include greater sensitivity after menopause, lower iron reserves and hormonal interactions.”}},{“@type”:”Question”,”name”:”How much hair loss on Ozempic is normal?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”It is normal to lose 50 to 100 hairs a day. With telogen effluvium it can be 200 to 300 or more. As long as the loss is diffuse (not patchy) and eases after the peak around month 4 to 6, it follows the expected course. Reasons to see a doctor are shedding beyond 6 months, patchy loss, scarring, or no regrowth after 12 months.”}},{“@type”:”Question”,”name”:”What type of hair loss does Ozempic cause?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”Predominantly a telogen effluvium: diffuse, temporary thinning across the whole scalp without bald patches, triggered by the stress of rapid weight loss. In people with a genetic predisposition, the weight-related telogen effluvium can additionally unmask an androgenetic alopecia, which shows up as patterned thinning. Rare cases of alopecia areata with round bald patches have been reported.”}},{“@type”:”Question”,”name”:”Should I stop Ozempic if I am losing hair?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”Not necessarily. For most people the hair loss is temporary, and stopping would cost you the therapeutic benefit, such as blood-sugar control, without any guarantee that your hair comes back faster as a result. Discuss it with the prescribing doctor. Stopping is only an option if the loss is severe, lasts beyond 12 months or is causing real distress, and only under medical supervision.”}},{“@type”:”Question”,”name”:”Does Ozempic damage the hair follicles directly?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”No, direct follicle damage from semaglutide is not proven. All the systematic reviews to date conclude that a causal link between the drug molecule and follicle toxicity is unproven. GLP-1 receptors have been detected in mouse hair follicles, but a functional expression in human follicles has not been confirmed. The hair loss is secondary to the metabolic stress of weight loss.”}},{“@type”:”Question”,”name”:”What is telogen effluvium?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”Telogen effluvium is a temporary form of hair loss in which a physiological stressor, such as rapid weight loss, surgery, illness or emotional strain, pushes many hair follicles prematurely into the resting phase. The result is diffuse hair loss around 2 to 3 months after the trigger. The follicles are not destroyed, and regrowth sets in once the stressor is removed. It is the most common mechanism behind GLP-1-related hair loss.”}}]} { “@context”: “https://schema.org”, “@type”: “MedicalWebPage”, “name”: “Does Ozempic Cause Hair Loss? Causes, FDA Data and What Really Helps Against Telogen Effluvium”, “url”: “https://elithair.com/blog/ozempic-hair-loss/”, “lastReviewed”: “2026-06-05”, “reviewedBy”: { “@type”: “Person”, “name”: “Dr. Imad Moustafa”, “jobTitle”: “Hair Transplant Physician”, “image”: “https://elithair.com/de/wp-content/uploads/sites/2/2026/05/dr-moustafa.webp”, “worksFor”: { “@type”: “MedicalOrganization”, “name”: “Elithair” } }, “author”: { “@type”: “Organization”, “name”: “Elithair” }, “about”: { “@type”: “MedicalCondition”, “name”: “Telogen Effluvium” } }
Dr. Imad Moustafa
Hair transplant specialist