
You have been injecting Mounjaro for a few months, the weight is finally coming off, and then this: more hair in the brush when you blow-dry, a worrying amount collecting in the drain. The worry kicks in right away. Does Mounjaro cause hair loss?
In short: Mounjaro and hair loss
Yes, Mounjaro can trigger hair loss, but not through any direct damage from the drug itself. The culprit is rapid weight loss, which sets off telogen effluvium, a diffuse and almost always reversible type of shedding. At the lower diabetes dose the risk is small; when used for weight loss at high doses it sits at around 5%.
- Cause: not the drug, but rapid weight loss. In the weight-loss trials around 4.9 to 5% of people were affected versus around 1% on placebo, and the FDA label classes alopecia as common (up to 1 in 10).
- Temporary and reversible: the follicles stay intact, and most people recover even without stopping treatment.
- Regrowth: typically visible after 6 to 12 months, once your weight and nutrient levels have settled. Women are affected more than men (7.1% vs 0.5%).
- When to see a doctor: if you notice bald patches, an irritated scalp, or a clear pattern that remains after 12 months.
Thousands of patients are asking themselves this very question, now that tirzepatide is widely prescribed both for type 2 diabetes (as Mounjaro) and for weight management (as Zepbound). Because tirzepatide is used so widely, the most reliable data on tirzepatide and hair loss come from the large weight-loss trials. The same drug, the same mechanism, so the findings apply to everyone taking it.
The short answer is this: yes, hair loss does happen on Mounjaro, but almost never in the way most people assume. The active ingredient, tirzepatide, does not attack the hair root directly. The culprit is the rapid weight loss itself, which triggers a temporary type of shedding called telogen effluvium. That is the crucial distinction: telogen effluvium is almost always reversible. In this article we go through the evidence on Mounjaro, put the figures from the approval trials and the FDA label into context, and tell you exactly what you can do about the shedding and when to take a closer look.
If your hair loss appears while you are on Mounjaro, the most likely explanation is the pace of your weight loss, not permanent damage. So do not stop the injections in a panic; get the situation assessed instead. When in doubt, a professional opinion is worth having before you change anything about your treatment.
Summary
- Does Mounjaro cause hair loss? What the studies show
- How does hair loss on Mounjaro show itself?
- Why Mounjaro costs you hair: the mechanism
- When does the hair loss start, and when does it stop?
- Who is most at risk
- Diabetes or weight loss: why the indication makes the difference
- Mounjaro and hereditary hair loss: a double-edged relationship
- How can I prevent hair loss on Mounjaro?
- What helps against the hair loss, and will the hair grow back?
- The Elithair approach: when a hair transplant makes sense
- Mounjaro compared with other GLP-1 medications
- When you should see a doctor: the warning signs
- Frequently asked questions about Mounjaro and hair loss
- Conclusion: does Mounjaro cause hair loss?
- Sources
Does Mounjaro cause hair loss? What the studies show
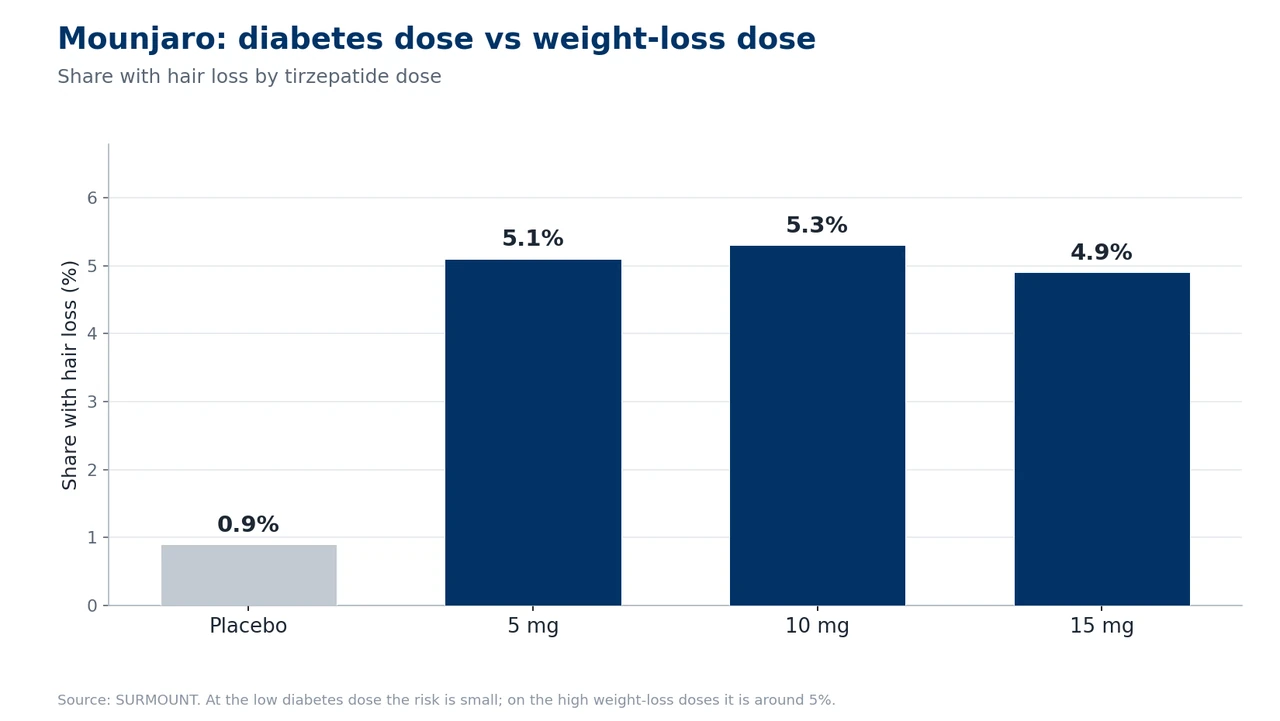
The most robust figures come from the weight-loss approval trials. In the SURMOUNT-1 trial, published in the New England Journal of Medicine in 2022 with 2,539 participants, hair loss was reported by 5.1% (5 mg), 5.3% (10 mg) and 4.9% (15 mg) of tirzepatide patients depending on the dose, compared with just 0.9% in the placebo group. That is a roughly fivefold increase in relative risk, but in absolute terms it still affects only a minority of those treated.
The official FDA Prescribing Information is what counts here. The label uses clear wording in its adverse-reactions section: hair loss was reported in 4.9% of patients treated with tirzepatide and in 1.0% on placebo. The events were mostly mild, the majority recovered while continuing treatment, and not a single patient stopped therapy because of the hair loss. The FDA therefore classes alopecia as “common,” meaning at least 1 in 100 but fewer than 1 in 10 of those treated.
An important point for understanding Mounjaro: these figures come from the weight-loss trials at the high doses. In the original diabetes trials (the SURPASS series) alopecia did not show up as a notable side effect at all, because weight loss there is far smaller. It was not until February 2025 that the FDA added hair loss retrospectively to the post-marketing observations section of the Mounjaro label. That underlines the point: the risk is tied to the degree of weight loss, not to the drug itself. You can read more about the shared active ingredient and how both brands work in our hub article on tirzepatide and hair loss.
The pharmacovigilance data paint a more nuanced picture too. A FAERS analysis by Godfrey and colleagues (JEADV 2025) found a significantly raised reporting signal for alopecia with tirzepatide (ROR 1.73), although lower than for semaglutide (ROR 2.46). A later, adjusted analysis by Lee and Kim (2026) found no significant signal at all for tirzepatide. Variation like this stems from different analytical models and observation periods, and it is a reminder to be cautious about individual spontaneous-reporting figures.
| Source | Context | Hair loss (tirzepatide) | Placebo |
|---|---|---|---|
| Mounjaro FDA label | Weight management | 4.9% (common) | 1.0% |
| SURMOUNT-1 (NEJM 2022) | Obesity, 15 mg | 4.9% | 0.9% |
| Zepbound FDA label (pooled) | Obesity, by sex | Women 7.1%, men 0.5% | Women 1.3%, men 0% |
| SURPASS (diabetes) | Type 2 diabetes | Not listed as a trial side effect | — |
How does hair loss on Mounjaro show itself?
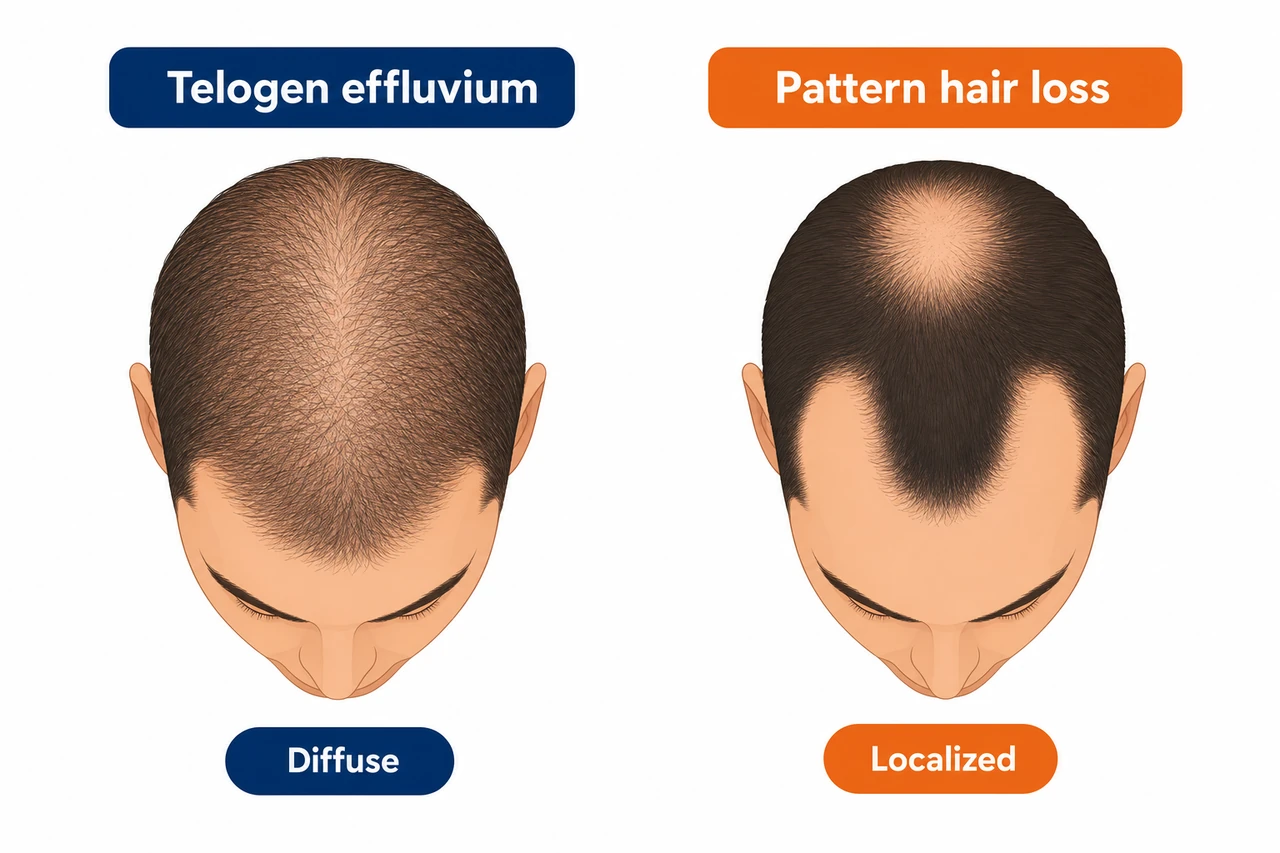
The typical pattern is diffuse thinning across the whole scalp, not a focal or patterned loss. You shed more hair evenly all over, without any particular zone such as the temples or the crown being especially affected. Instead of the normal 100 or so hairs a day, with telogen effluvium it can be 200 to 300 or more.
A cross-sectional study by Argobi and colleagues (2026) of 254 GLP-1 users gives some concrete figures: 29.5% of those affected lost an extra 50 to 100 hairs a day, 43.5% rated their hair loss as moderate, and 35.8% as severe. In 86% the classic telogen pattern was seen, that is, hairs that fall out together with the pale bulb at the root. That is a strong indication that this is telogen effluvium and not broken hairs.
What to look out for: with telogen effluvium the scalp is calm, so no redness, no itching, no flaking. If you develop round bald patches, or burning or painful spots, that points to a different cause. There is more on this in the warning-signs section further down. For how a diffuse type of hair loss differs in principle from patterned forms, we explain it in detail in our foundational article.
Why Mounjaro costs you hair: the mechanism
To judge the risk properly, it helps to look at the biology. Mounjaro (tirzepatide) is a dual GIP and GLP-1 receptor agonist that curbs the appetite and brings about substantial weight loss. In SURMOUNT-1, participants on 15 mg lost around 20.9% of their body weight over 72 weeks. It is precisely this rapid, marked weight loss that is the real trigger for the hair loss.
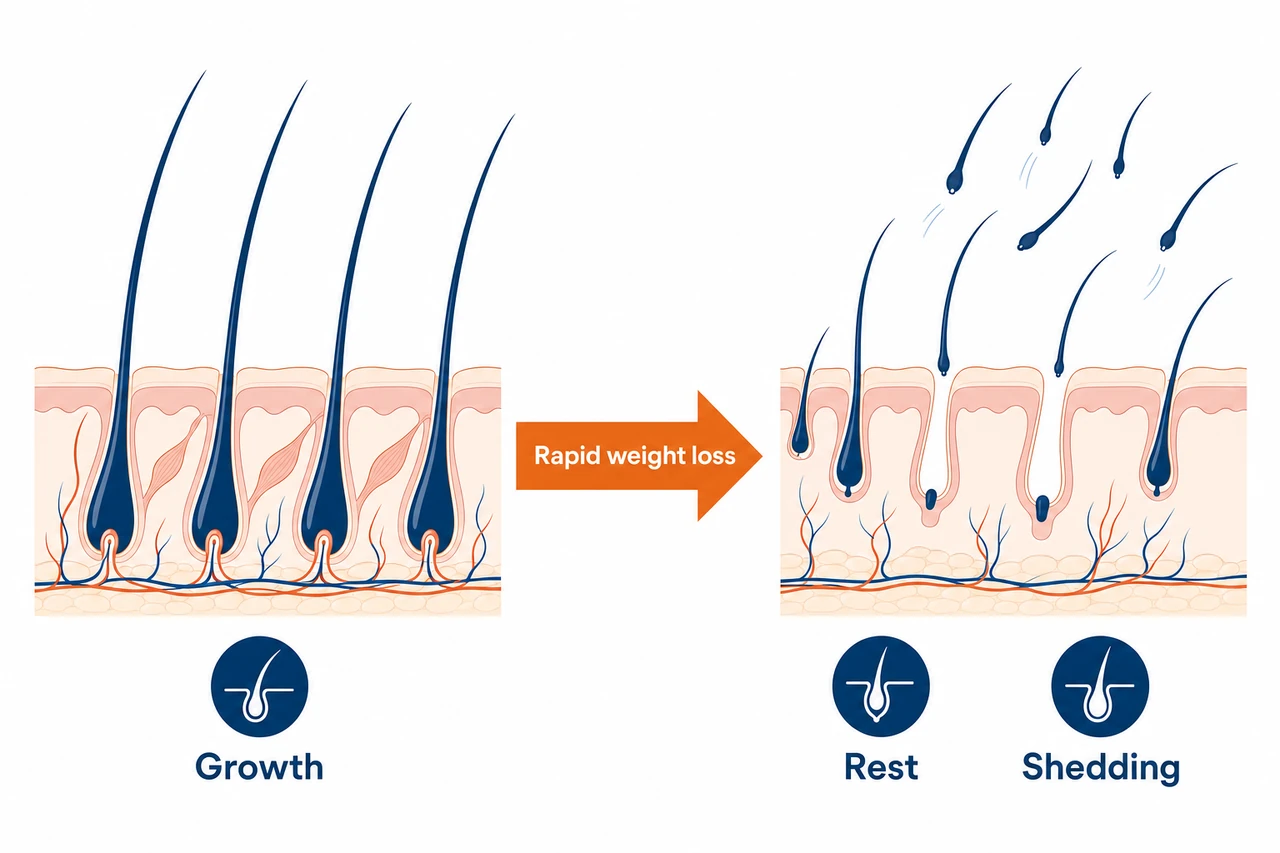
The body reads a large calorie deficit and rapid weight loss as physiological stress. Hair growth is not an essential function, so the body dials it down and redirects energy and nutrients to the vital organs. The result: an unusually large number of hair follicles shift from the growth phase into the resting phase all at once. Normally 5 to 10% of follicles are in telogen; with telogen effluvium it can be 30 to 70%. Because a hair does not fall out until around two to four months after it enters the resting phase, you notice the shedding with a delay. If you want to know more about the phases, you will find the details in our article on the hair growth cycle.
This is all made worse by nutrient deficiencies. On Mounjaro you simply eat less because your appetite is suppressed, and that often means a lower intake of protein, iron, zinc and vitamin D, all of which are central to the hair root. Hair is around 90% keratin, a protein. If protein intake falls too low, the risk of telogen effluvium rises sharply. In one analysis of Mounjaro hair-loss patients, 88.4% had an iron deficiency and almost all had an inadequate vitamin D level.
The decisive point: there is no evidence that tirzepatide is directly toxic to the follicle. Recent review papers stress this explicitly. The best proof is the discrepancy between the indications. At the diabetes dose, with less weight loss, hair loss barely occurs; at the obesity dose, with dramatic weight loss, it affects around 5%. If the drug were directly harmful, the effect would have to be similar in both groups. It is not.
When does the hair loss start, and when does it stop?
Telogen effluvium follows a predictable course. The shedding typically begins 2 to 4 months after starting treatment or after a dose increase, not right away. In the Argobi 2026 study, 38.8% of those affected reported an onset within the first 1 to 3 months.
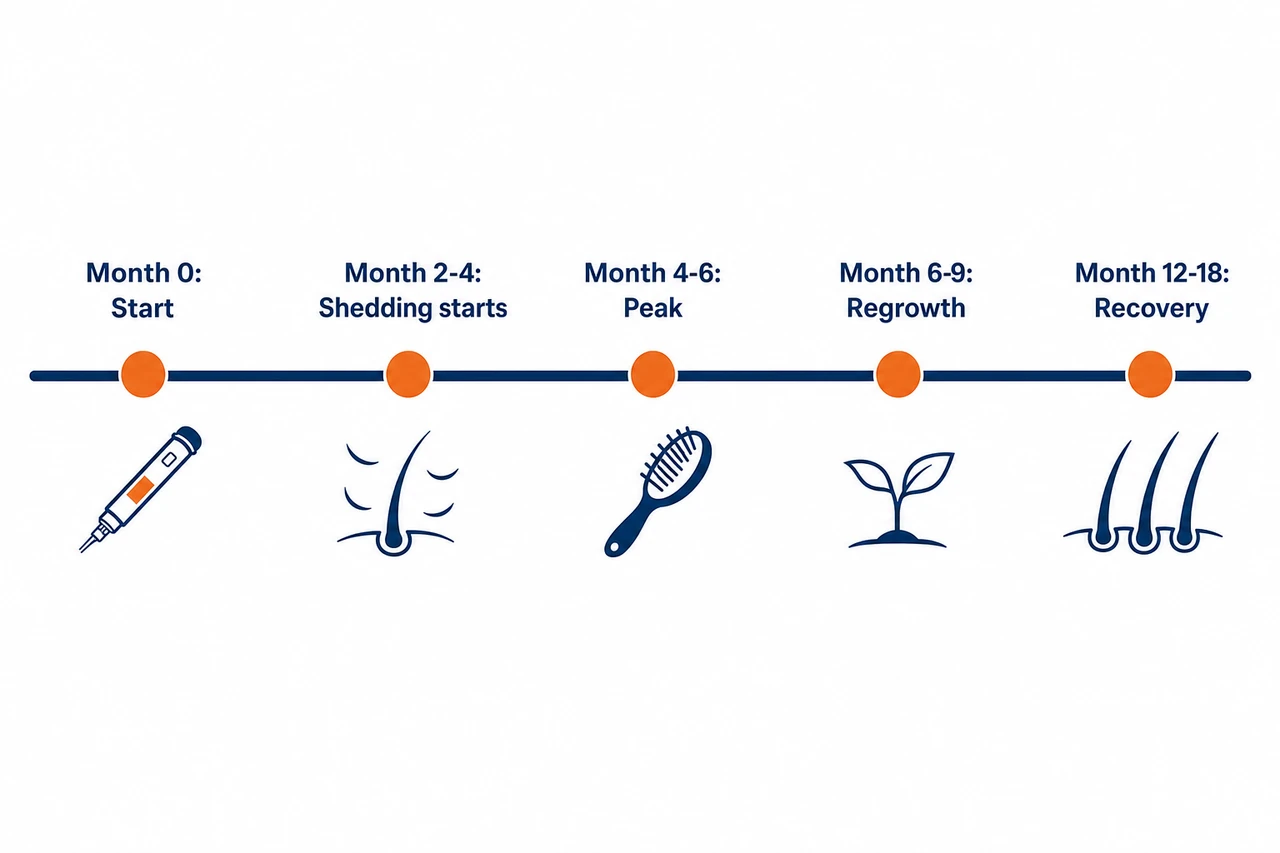
The shedding phase that follows usually lasts 3 to 6 months. There is one peculiarity with Mounjaro: because the weight loss can carry on for more than 72 weeks, the phase sometimes drags on longer than with classic acute telogen effluvium. Recovery begins as your weight stabilizes and your diet improves. The first regrowth, in the form of short baby hairs, is typically visible after 3 to 6 months, with a cosmetically meaningful return of hair after 6 to 12 months.
Crucial and reassuring at the same time: the FDA label records that most patients recovered while continuing treatment. So you do not necessarily have to stop Mounjaro for your hair to come back, once your body has adjusted to its new weight. If, however, the hair loss persists for 6 to 12 months with no sign of recovery, that points to a different, permanent cause. A dermatological assessment is then worthwhile.
Who is most at risk
Not every Mounjaro user loses hair. Your personal risk depends on several factors, and the most important is not the dose as such but how much and how quickly you lose weight.
- Extent of weight loss. The single strongest factor. Patients who lost more than 20% of their weight had an alopecia rate of 5.3% compared with 2.5% in those who lost under 20%. Anyone using Mounjaro for weight loss who loses a lot is far more likely to be affected than a diabetes patient with moderate loss.
- Sex. Women are clearly more affected: 7.1% compared with 0.5% in men in the pooled tirzepatide data. In the Argobi study, men were 64% less likely to experience hair loss.
- Pace of dose escalation. Titrating up to 15 mg quickly means a sharper calorie restriction and so more stress for the hair. The standard schedule, with a step up every 4 weeks, is the more sensible route here.
- Indication. The weight-loss indication carries a markedly higher risk than diabetes treatment alone, because diabetes patients often receive lower doses and lose less weight.
- Pre-existing deficiencies. Low baseline ferritin and iron, zinc or vitamin D deficiency raise the risk. People who are overweight often already have suboptimal micronutrient levels before treatment begins.
- Family predisposition. In one analysis, 91.4% of those affected already had a personal history of hair loss. A family tendency toward hereditary hair loss is a risk factor.
Diabetes or weight loss: why the indication makes the difference
Mounjaro is a special case, because tirzepatide stands behind two very different situations. Tirzepatide was originally approved for type 2 diabetes as Mounjaro (FDA approval May 2022). It is also approved for chronic weight management, marketed as Zepbound (FDA approval November 2023). That weight-loss setting is exactly where hair loss becomes an issue.
The reason is the difference in weight loss. Diabetes patients in the SURPASS trials lost around 8 to 11% of their body weight. Patients in the obesity indication, on the higher doses, lose around 21%. More weight loss means more metabolic stress and so more telogen effluvium. That is why hair loss is barely an issue in the diabetes trials, yet a common side effect in the weight-loss trials.
In practical terms for you: if you take Mounjaro for diabetes at a lower dose and lose only moderate weight, your risk is small. If you use tirzepatide for weight loss at high doses and lose a lot of weight, shedding is more likely, but it is still reversible. This is also the heart of the difference from its identical sister product Zepbound, which is marketed solely for the obesity indication at high doses and accordingly shows higher hair-loss rates.
Mounjaro and hereditary hair loss: a double-edged relationship
This is where it gets interesting, because, paradoxically, Mounjaro can affect your hair in two opposite directions. On the one hand, rapid weight loss can unmask or accelerate a previously invisible, genetically driven androgenetic alopecia. A large TriNetX cohort of almost 548,000 matched patients showed that, at 12 months, GLP-1 users had a raised risk not only of telogen effluvium but also of androgenetic alopecia (around 1.6-fold). So if the hair loss does not ease off after 6 to 12 months but instead takes on a clear pattern (a receding hairline, a thinning crown), an unmasked predisposition may be behind it.
On the other hand, there is a surprising finding. A published case report (Gordon et al., JAAD Case Reports 2024) documented a marked improvement in hair density on tirzepatide in a 57-year-old man with androgenetic alopecia and insulin resistance, without any additional hair-growth treatments. The mechanism: tirzepatide lowers insulin resistance, and high insulin secretion is regarded as a driver of follicle miniaturization, partly through stronger androgen signaling and more DHT production. This is, however, a single case and cannot be generalized. We go deeper into how hormones such as DHT govern hair loss in our article on hormones and hair.
What this means in practice: if your telogen effluvium recovers but a pattern remains, a latent predisposition has probably become visible. Where you sit on the Norwood-Hamilton scale can then be assessed professionally and treated in a targeted way.
The key fork in the road: diffuse or patterned?
Diffuse loss across the whole scalp (telogen effluvium): reversible, no hair transplant needed. Give your hair 6 to 12 months, eat 1.2 to 1.6 g of protein per kilogram of body weight, have your ferritin checked (target above 70 ng/mL), and do not stop Mounjaro abruptly; at most taper it gradually with your doctor.
Patterned loss at the temples and crown (unmasked hereditary alopecia): if rapid weight loss has revealed an androgenetic alopecia that was already there, these follicles will not recover on their own. This is the case for a permanent solution.
Not sure which type you have? That is exactly what a free hair analysis clarifies. In a few minutes you will know whether your loss is temporary or is taking on a permanent pattern, before you change anything about your treatment.
How can I prevent hair loss on Mounjaro?
You can actively lower the risk. The common thread: give your body enough building blocks despite the appetite suppression, and do not push the pace of weight loss too hard.
The most effective protective measures:
- ✅ Enough protein. Aim for 1.2 to 1.6 g per kilogram of body weight a day, at least 60 to 80 g in absolute terms, spread across several meals. If your appetite is low, eggs, fish, beans, Greek yogurt or protein shakes can help.
- ✅ Check your micronutrients. Before you start and every 3 to 6 months, have your ferritin, zinc, vitamin D, B12 and thyroid levels measured and correct any deficiencies in a targeted way. For robust hair growth, ferritin should be above 70 ng/mL.
- ✅ Titrate slowly. Stick to the standard schedule (one step every 4 weeks). If shedding starts after a dose increase, discuss pausing further escalation with your doctor until your nutritional status is right.
- ✅ Ease off the pace. Losing a maximum of 0.5 to 1 kg a week is gentler on the hair than a crash. Faster loss raises the risk.
- ✅ Be kind to your hair. During the shedding phase, avoid aggressive heat styling, tight hairstyles and harsh shampoos.
One important note on the often-recommended biotin: in people without a biotin deficiency it does nothing for hair growth. High-dose biotin can also distort certain blood tests (such as troponin or TSH) and should be stopped before lab work. Better to save your money for a balanced protein intake.
What helps against the hair loss, and will the hair grow back?
If the hair loss is already under way, you can soften its pace and extent. The foundation is always to address the cause, that is, stabilize your weight and correct nutrient deficiencies. In many cases that alone already improves the course.
- Correct deficiencies. Address a proven iron, ferritin, zinc or vitamin D deficiency in a targeted way. With zinc deficiency, case series have even described a complete resolution of telogen effluvium.
- Topical minoxidil 5%. A sensible option for persistent shedding. An open study of crash-diet-related telogen effluvium showed a markedly higher hair density and 100% patient satisfaction after 24 weeks. It works by improving blood flow and prolonging the growth phase.
- Oral low-dose minoxidil. Off-label and only under medical supervision. In studies it improved or stabilized hair status in the majority of patients.
- PRP (platelet-rich plasma therapy). A meta-analysis of 21 randomized studies showed a significant improvement in hair density and thickness. At Elithair it is part of the treatment offering and can be used as a supportive measure during the growth phase.
For diffuse hair loss that lasts longer than 3 months, a dermatological examination with trichoscopy is worthwhile, to rule out androgenetic alopecia, scarring alopecia or alopecia areata. Oral minoxidil belongs in medical hands in any case.
Many patients come to us in a panic because they are losing hair on their weight-loss injection. What they are usually experiencing is telogen effluvium, a reaction to rapid weight loss, not damage from the medicine itself. The follicles are intact, and the hair almost always comes back. The important thing is not to stop the injection out of fear on your own, to adjust your diet, and to be patient. Only if a clear pattern remains after about a year is it worth taking a close look at a hereditary component.
Dr. Balwi, Medical Director at Elithair
The Elithair approach: when a hair transplant makes sense
One thing first, because it takes a lot of worry away: with pure telogen effluvium caused by Mounjaro, a hair transplant is not needed and is in fact contraindicated. The follicles are intact and only temporarily in the resting phase. Here the rule is: wait, optimize your diet, use minoxidil or PRP if needed, and give your hair up to 12 months.
A hair transplant only becomes relevant once, after 12 months of stable weight and an optimized diet, a clear androgenetic pattern remains (a receding hairline, a thinned crown) and trichoscopy confirms an unmasked predisposition. These miniaturized follicles will then no longer recover on their own. Timing is key: no transplant while your weight is still actively falling or your hair loss has not stabilized.
Elithair has carried out more than 150,000 hair transplants, works to TÜV-certified ISO 9001 standards and gives a written 20-year guarantee. As standard we use the DHI method, supplemented by NEO FUE, a plant-based stem-cell serum that raises the graft survival rate to up to 98%. The transplanted hair comes from the DHT-resistant donor area and therefore does not fall out again. But the first and decisive step is always the same: finding out whether your loss is reversible or not.
Mounjaro compared with other GLP-1 medications
How does Mounjaro stack up against the other weight-loss and diabetes injections? The table below shows that the greater a medication’s average weight loss, the higher the hair-loss signal tends to be.
| Medication | Active ingredient | Indication | Hair loss (active drug) | Placebo |
|---|---|---|---|---|
| Mounjaro | Tirzepatide | Diabetes (US) | far lower for diabetes | ~1% |
| Zepbound | Tirzepatide | Weight loss (US) | 5% (women 7.1%, men 0.5%) | 1% |
| Wegovy | Semaglutide 2.4 mg | Weight loss | 3.3% (women 4%, men 0.9%) | 1% |
| Ozempic | Semaglutide 0.5−2 mg | Diabetes | Not listed as a trial side effect | — |
To put this in context: tirzepatide (Mounjaro and Zepbound) and high-dose semaglutide (Wegovy) show the strongest signals, because they produce the greatest weight loss (tirzepatide around 21%, Wegovy around 15%). The diabetes counterparts Ozempic (semaglutide) and low-dose tirzepatide barely trigger any hair loss, because the weight loss is more moderate. A 2026 cross-sectional study did find particularly high odds of severe hair loss among Mounjaro users, but in that cohort every participant was taking the medication for weight loss, so in the high-dose situation. The common denominator across all the brands is always the same: the pace of weight loss.
When you should see a doctor: the warning signs
Telogen effluvium is harmless and temporary. There are, however, situations where you should not wait but get a professional assessment.
Round or oval bald patches (suspected alopecia areata), redness, burning or itching of the scalp alongside hair loss (suspected scarring alopecia, which can be irreversible if left untreated), or sudden swelling or pustules.
Hair loss persisting for more than 6 months without slowing, a clear pattern emerging (frontal recession, crown thinning), or no regrowth after 12 months despite stable weight. Your doctor is the first place to start.
Sensible baseline tests at the doctor’s: a complete blood count, ferritin, transferrin saturation, thyroid levels (TSH, fT4), zinc, vitamin D, B12 and HbA1c. For women where a hormonal cause is suspected, androgen levels as well.
Frequently asked questions about Mounjaro and hair loss
Conclusion: does Mounjaro cause hair loss?
Yes, but with one important caveat. Mounjaro does not attack your hair roots directly. The hair loss is telogen effluvium, the body’s stress reaction to rapid weight loss, and so it is almost always temporary and reversible. The risk depends on how much weight you lose: barely an issue at the diabetes dose, around 5% when losing weight at high doses. Women are affected more than men. With enough protein, balanced micronutrients and a pace of weight loss that is not pushed too hard, you can noticeably lower the risk. Do not stop the injections in a panic; when in doubt, get your hair status checked. Only if a clear pattern remains after about a year is it worth taking a close look at a hereditary cause.
Sources
- Mounjaro UK Summary of Product Characteristics (SmPC), section 4.8, medicines.org.uk. medicines.org.uk
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). N Engl J Med. 2022. NEJM
- Zepbound (tirzepatide) FDA Prescribing Information, NDA 217806, section 6.1, 2024. accessdata.fda.gov
- Mounjaro (tirzepatide) FDA Prescribing Information with post-marketing addition, NDA 215866s031, Feb 2025. accessdata.fda.gov
- Frías JP, Davies MJ, Rosenstock J, et al. Tirzepatide versus Semaglutide Once Weekly (SURPASS-2). N Engl J Med. 2021. NEJM
- Gupta AK, Teasell EM, Economopoulos V, Mirmirani P. GLP-1 therapies and hair loss: A systematic review. Science Progress. 2026. Sage
- Argobi Y, Jadaan NS, et al. Predictors and Characteristics of Hair Loss Among Users of GLP-1 Receptor Agonists. J Cosmet Dermatol. 2026. PMC
- Vidal SI, Akiska YM, Nasseri M, et al. Increased risk of hair loss with GLP-1 receptor agonists: TriNetX cohort study (n=547,993). JAAD International. 2026. PMC
- Godfrey H, Leibovit-Reiben Z, Jedlowski P, Thiede R. Alopecia associated with semaglutide and tirzepatide: A FAERS disproportionality analysis. J Eur Acad Dermatol Venereol. 2025. PubMed
- Gordon ER, Musleh S, Bordone LA. Treatment of insulin resistance with tirzepatide leading to improvement of hair loss. JAAD Case Reports. 2024. PMC
- American Academy of Dermatology. How can GLP-1 drugs affect my skin, hair, and nails? 2026. aad.org
- Telogen Effluvium. StatPearls, NIH/NCBI Bookshelf. 2024. NCBI
This article is for information only and does not replace medical advice. Speak to your doctor, your prescriber or a dermatologist before making any change to your medication or treatment. If hair loss persists, you should seek a professional diagnosis.
{“@context”:”https://schema.org”,”@type”:”FAQPage”,”mainEntity”:[{“@type”:”Question”,”name”:”Does Mounjaro cause hair loss?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”Yes, in some people. In the weight-loss trials, hair loss occurred in around 5% of tirzepatide patients, compared with around 1% on placebo. The FDA classes it as a common side effect. The cause is not the medication directly, but rapid weight loss, which triggers telogen effluvium. Most people recover even without stopping treatment.”}}, {“@type”:”Question”,”name”:”Will my hair grow back after Mounjaro hair loss?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”In most cases, yes. Telogen effluvium is reversible and the follicles are intact. Once your weight stabilizes and your nutrient status is right, regrowth typically begins after 3 to 6 months, with a cosmetically visible effect after 6 to 12 months. The FDA label confirms that most patients recover while continuing treatment.”}},{“@type”:”Question”,”name”:”Do women lose more hair on Mounjaro than men?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”Yes, considerably. In the tirzepatide data, 7.1% of women reported hair loss, but only 0.5% of men. A 2026 cross-sectional study found that men were 64% less likely to experience hair loss. Women are generally more prone to telogen effluvium.”}},{“@type”:”Question”,”name”:”How can I prevent hair loss on Mounjaro?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”Eat enough protein (1.2 to 1.6 g per kilogram a day), have your ferritin, zinc and vitamin D measured before and during treatment and correct any deficiencies, stick to the standard titration schedule, avoid losing weight too quickly, and be gentle with your hair when styling. For heavy shedding, topical minoxidil 5% can help.”}},{“@type”:”Question”,”name”:”Which vitamins and nutrients help against Mounjaro hair loss?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”The key ones are iron (ferritin ideally above 70 ng/mL), zinc, vitamin D and, above all, enough protein, since hair is around 90% keratin. Have your levels measured with a blood test and correct only proven deficiencies in a targeted way. Taking supplements at random does nothing. Biotin is ineffective in people without a deficiency and can also distort blood tests.”}},{“@type”:”Question”,”name”:”Should I stop Mounjaro if I am losing hair?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”In most cases this is not necessary. The FDA label records that most patients recover even while continuing treatment. If you stop Mounjaro and quickly regain weight, that can even trigger a fresh round of telogen effluvium. You should make any decision to stop with your doctor, based on the overall benefit, not on the hair alone.”}},{“@type”:”Question”,”name”:”When does the hair loss start after starting Mounjaro?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”Typically 2 to 4 months after starting treatment or after a dose increase, not right away. This delay is normal, because a hair does not fall out until around three months after it enters the resting phase. In a 2026 study, 38.8% of those affected reported an onset within the first 1 to 3 months.”}},{“@type”:”Question”,”name”:”Does Mounjaro cause more hair loss than other GLP-1 medications?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”At the weight-loss doses, tirzepatide (Mounjaro and Zepbound) appears to trigger slightly more hair loss than Wegovy (semaglutide), around 5% versus 3%, because tirzepatide produces more weight loss on average (around 21% vs 15%). At the lower diabetes dose the risk is much smaller. The decisive factor is always the extent of weight loss.”}},{“@type”:”Question”,”name”:”Why is the risk lower with diabetes than with weight loss?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”Because weight loss is what tips the balance. Diabetes patients lose around 8 to 11% of their body weight in the trials, while weight-loss patients on the higher doses lose around 21%. More and faster loss means more metabolic stress and so more telogen effluvium. That is why hair loss barely appears in the diabetes-only trials.”}},{“@type”:”Question”,”name”:”Can Mounjaro also promote hair growth?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”In isolated cases, paradoxically, yes. A 2024 case report documented a marked improvement in hair density on tirzepatide in a man with hereditary hair loss and insulin resistance. By lowering insulin resistance, the hormonal drivers of follicle miniaturization were reduced. This is, however, a single case and cannot be generalized.”}},{“@type”:”Question”,”name”:”Do I need a hair transplant if I lose hair on Mounjaro?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”With pure telogen effluvium, no. It is reversible and the follicles recover on their own. A hair transplant only becomes relevant once, after around 12 months of stable weight, a clear hereditary pattern remains and trichoscopy confirms an unmasked androgenetic alopecia.”}},{“@type”:”Question”,”name”:”When should I see a doctor about hair loss on Mounjaro?”,”acceptedAnswer”:{“@type”:”Answer”,”text”:”See a doctor if the hair loss is patchy or shows round bald spots, if the scalp is red or itchy, if the shedding persists for more than 6 months without slowing, if a clear pattern is forming, or if you are considering prescription treatments such as oral minoxidil. Your doctor is the first place to start.”}}]} { “@context”: “https://schema.org”, “@type”: “MedicalWebPage”, “name”: “Mounjaro and Hair Loss: Does Tirzepatide Cause Hair Loss and Will It Grow Back?”, “url”: “https://elithair.com/blog/mounjaro-hair-loss/”, “lastReviewed”: “2026-06-05”, “reviewedBy”: { “@type”: “Person”, “name”: “Dr. Imad Moustafa”, “jobTitle”: “Hair Transplant Physician”, “image”: “https://elithair.com/de/wp-content/uploads/sites/2/2026/05/dr-moustafa.webp”, “worksFor”: { “@type”: “MedicalOrganization”, “name”: “Elithair” } }, “author”: { “@type”: “Organization”, “name”: “Elithair” }, “about”: { “@type”: “MedicalCondition”, “name”: “Telogen Effluvium” } }
Dr. Imad Moustafa
Hair transplant specialist