
Medically reviewed by Dr. Imad Moustafa, hair transplant specialist. Updated June 2026.
If you have been losing hair, you have probably run into the term “DHT blocker” already. Forums push them, supplement brands sell them, and your barber might have an opinion too. So what actually works, what is hype, and what should you be careful with? This guide walks through how the hormone behind most hair loss works, what the real options are (prescription, natural, and topical), who they suit, and when a hair transplant becomes the more honest answer.
What is a DHT blocker? A DHT blocker is any treatment that lowers dihydrotestosterone (DHT), the hormone that shrinks genetically sensitive hair follicles. Most work by inhibiting the enzyme 5-alpha-reductase, which converts testosterone into DHT. Options range from prescription tablets like finasteride to natural extracts and medicated shampoos.
- The strongest DHT blockers are the prescription 5-alpha-reductase inhibitors finasteride and dutasteride. Everything else is weaker.
- Natural options like saw palmetto and pumpkin seed oil have a mild effect at best. They are not a like-for-like swap for medication.
- Topical versions and ketoconazole shampoo work on the scalp with far less drug in the bloodstream, useful if systemic side effects worry you.
- DHT blockers manage hair loss, they do not cure it. Stop taking them and the loss resumes.
- After a hair transplant, a DHT blocker protects your native (non-transplanted) hair, which keeps the overall result looking natural for years.
Summary
- What is DHT and how does it affect hair growth?
- How do DHT blockers actually work?
- The main prescription options: finasteride and dutasteride
- Topical finasteride and dutasteride
- DHT-blocker shampoos and ketoconazole
- Natural DHT blockers: supplements and how strong the evidence is
- Foods that act as natural 5-alpha-reductase inhibitors
- How to lower DHT naturally
- Comparison table: prescription vs natural vs topical
- Side effects and safety
- Who are DHT blockers for?
- How long do DHT blockers take to work?
- Do I need DHT blockers after a hair transplant?
- Alternatives to DHT blockers
- FAQ
- Sources
What is DHT and how does it affect hair growth?
Dihydrotestosterone (DHT) is an androgen made from testosterone. Testosterone drives a lot of male traits, the deeper voice, body hair, muscle mass. DHT is its more potent cousin: it binds to androgen receptors with markedly higher affinity than testosterone and holds on longer, and it does more damage where hair is concerned.
The body converts testosterone into DHT using an enzyme called 5-alpha-reductase. There are two forms of it. Type I sits in skin and sebaceous glands across the body. Type II is the one that matters for hair: it concentrates in the dermal papilla of scalp follicles and accounts for most of the DHT produced near the hair root.
In people with a genetic sensitivity, DHT binds to receptors inside the follicle and gradually miniaturizes it. With each growth cycle:
- the hair comes back finer,
- the growing (anagen) phase shortens,
- the resting phase lengthens,
- and eventually the follicle produces little more than fuzz.
That is androgenetic alopecia, male and female pattern hair loss.
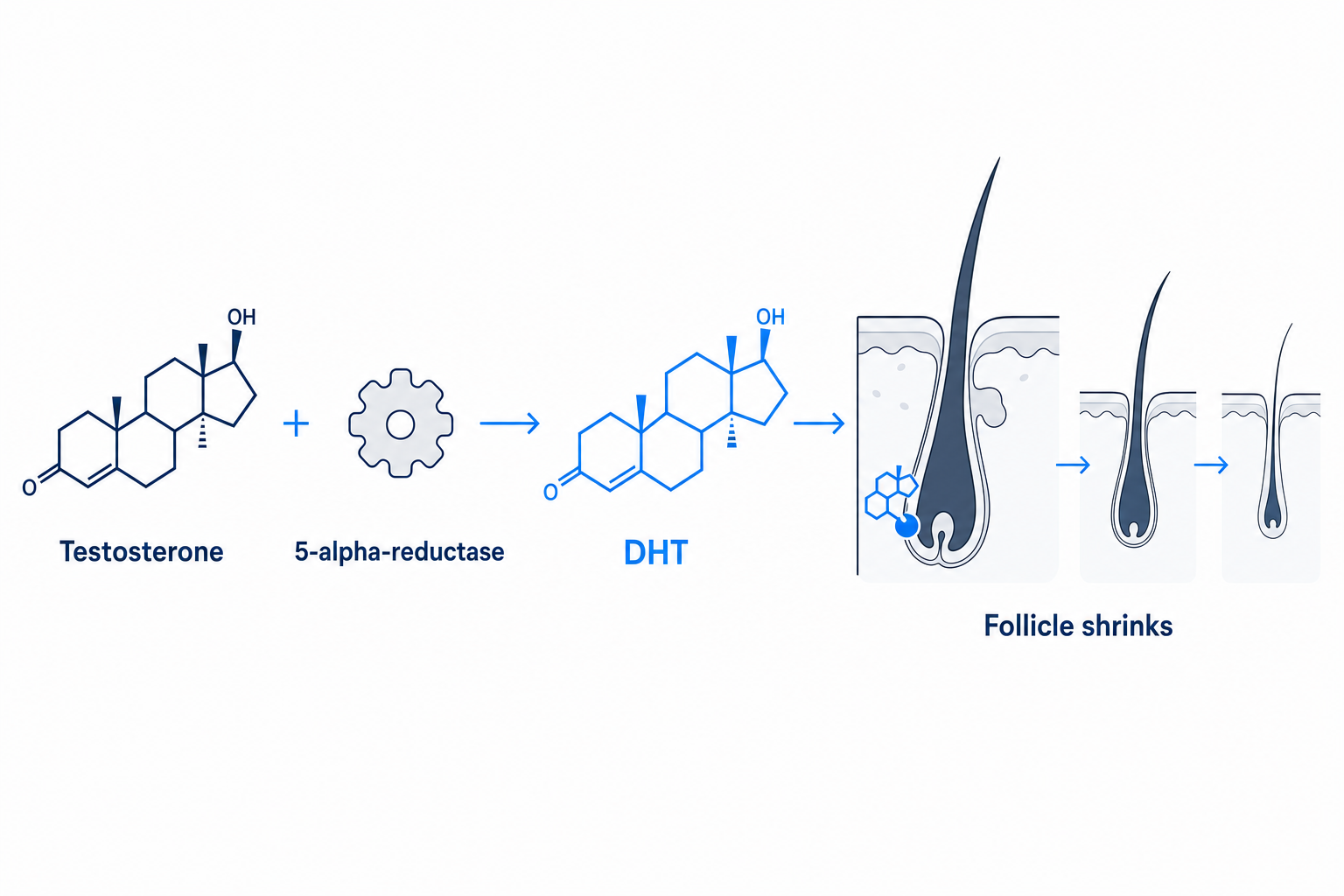
Testosterone is converted by 5-alpha-reductase into DHT, which binds to the follicle and gradually shrinks it.
The pattern itself, receding temples and a thinning crown, simply reflects where follicles carry the most androgen receptors and Type II activity. The hair at the back and sides is naturally DHT-resistant, which is exactly why surgeons take donor grafts from there.
One detail worth knowing, because it trips up a lot of people: a normal blood DHT result does not mean you are in the clear. Serum DHT measured in a blood test does not reliably track how aggressive your hair loss is. What counts is the DHT produced locally inside the follicle, and balding scalp has measurably more of it than non-balding scalp even when blood levels look normal.
How do DHT blockers actually work?
“DHT blocker” is the everyday term, and it covers two genuinely different mechanisms. The distinction matters once you start comparing options.
The first approach cuts DHT at the source. Finasteride and dutasteride are 5-alpha-reductase inhibitors: they sit on the enzyme so less testosterone gets converted into DHT in the first place. Less enzyme activity, less DHT, less pressure on the follicle. These are the drugs most people mean when they say “DHT blocker,” even though, strictly speaking, they inhibit production rather than block the hormone itself.
The second approach blocks DHT at the receptor. Drugs like spironolactone occupy the androgen receptor so DHT cannot dock and signal the follicle to shrink. DHT levels stay the same, but the message does not get through. This class is mainly used in women (more on that below).
Most natural options, saw palmetto, pumpkin seed oil, nettle, lean toward the first mechanism, weakly inhibiting 5-alpha-reductase. The honest summary: prescription drugs do this strongly, plants do it gently, and the gap between them is large.
The main prescription options: finasteride and dutasteride
These are the most potent DHT blockers available, and the only ones with large clinical trials behind them. Neither is “the best” in any universal sense; the right choice depends on your hair loss, your tolerance for side effects, and a conversation with a doctor.
Finasteride 1 mg
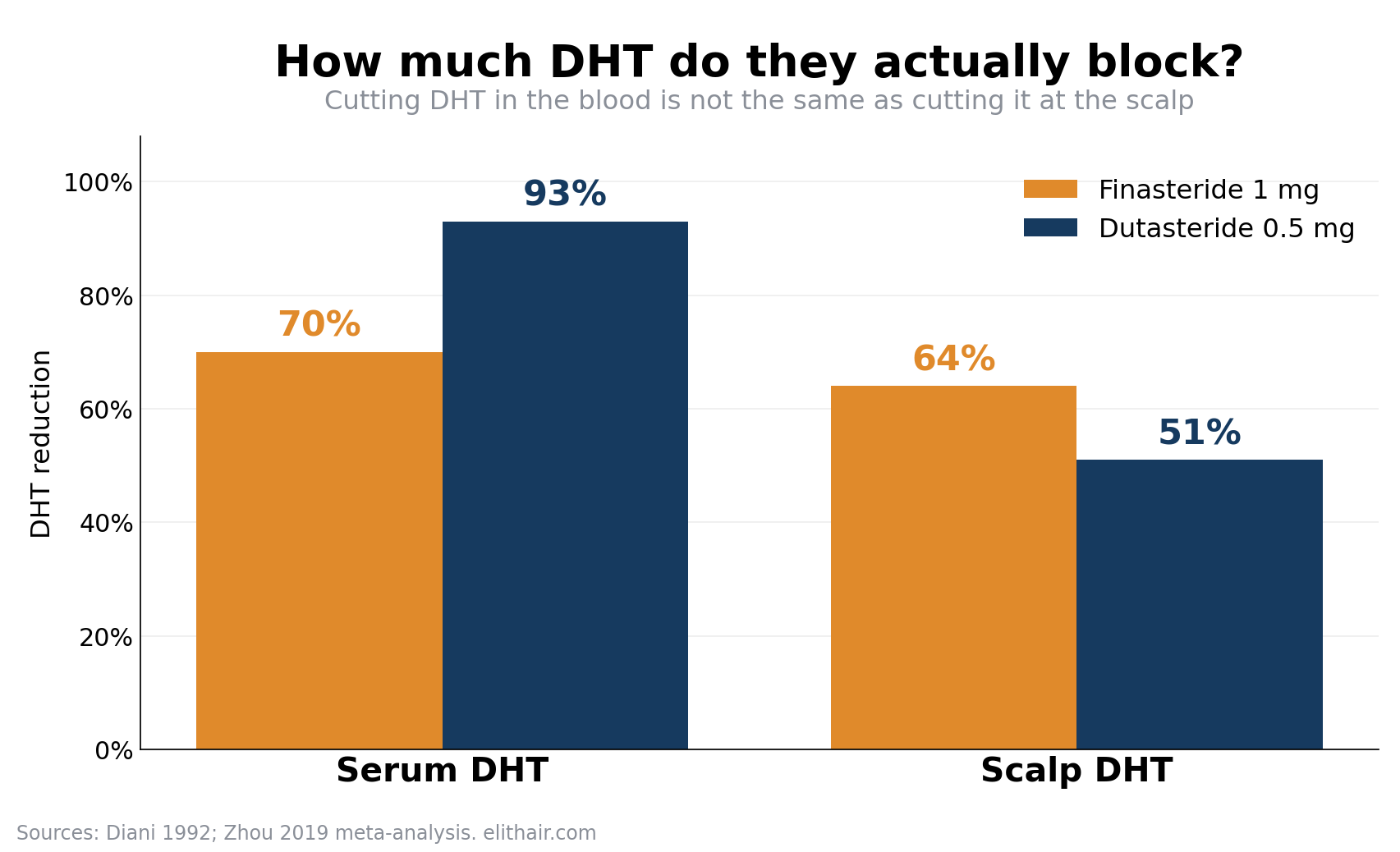
Finasteride blocks Type II 5-alpha-reductase. At 1 mg a day it lowers serum DHT by about 70% and scalp DHT by roughly 64%. In the registration trials it stopped further loss in around 83% of men and produced visible regrowth in about 65% at 12 months. It is licensed for male pattern hair loss in the US, the EU, and the UK.
Dutasteride 0.5 mg
Dutasteride goes further. It blocks both Type I and Type II 5-alpha-reductase, dropping serum DHT by around 92 to 95%. You would expect that to translate into far better hair results, but the picture is more nuanced: scalp DHT falls by only about 51%, not hugely more than finasteride, because the follicle relies so heavily on Type II anyway. In head-to-head trials dutasteride did edge out finasteride, producing on average about 29 more hairs over 24 weeks in a meta-analysis of three RCTs.
The catch is licensing. Dutasteride is approved for hair loss in South Korea, Japan, and Taiwan. In the US and UK it is only approved for an enlarged prostate, so any use for hair is off-label. That does not make it unsafe or unusual (doctors prescribe it off-label routinely), but you should know what you are signing up for.
Pregnancy warning, non-negotiable. Women who are pregnant or could become pregnant must not handle crushed or broken finasteride or dutasteride tablets. The drug can be absorbed through the skin and can cause abnormalities in the genitals of a male fetus. Intact, film-coated tablets are low risk; broken ones are not. Dutasteride carries the same warning and has a very long half-life.
Topical finasteride and dutasteride
If your main worry is systemic side effects, this is the section to read. Topical versions deliver the same active drugs to the scalp while keeping far less in the bloodstream.
In a phase III trial, topical finasteride spray put more than 100 times less drug into the blood than the oral tablet, and reduced serum DHT by about 35% versus roughly 56% for oral, yet scalp DHT dropped meaningfully in both and hair-count results were comparable. Sexual side effects ran lower too: about 2.8% with topical versus 4.8% with oral, and no one quit the topical arm because of them. Topical dutasteride shows a similar story in early trials, scalp efficacy with minimal systemic absorption.
Two honest caveats. First, no topical finasteride or dutasteride product is fully approved by the FDA yet, so what you find is usually compounded by a pharmacy, and quality varies. Second, the FDA warned in 2025 that compounded topical finasteride can still carry systemic risk, and the same pregnancy precaution applies. Lower exposure is not zero exposure.
DHT-blocker shampoos and ketoconazole
Shampoos sit at the gentle end of the scale. They cannot raise or lower the DHT in your blood; whatever they do happens on the scalp, and it washes off.
The one with real research behind it is ketoconazole 2%. It inhibits Type I 5-alpha-reductase locally and tamps down sebum, where some follicular DHT is produced. Based on their complementary mechanisms, researchers have proposed that ketoconazole shampoo added to finasteride could work better than finasteride alone, though no head-to-head trial has tested the combination yet. An older study even found 2% ketoconazole roughly comparable to 2% minoxidil on some measures, though the sample was tiny and the trial had clear limitations.
Keep expectations grounded. Ketoconazole shampoo is approved for dandruff and seborrheic dermatitis, not hair loss. Think of it as a useful supporting act for scalp health alongside a real treatment, not a replacement for one.
Natural DHT blockers: supplements and how strong the evidence is
This is where the internet gets carried away. Natural options can have a mild anti-androgenic effect, and some have a decent single study behind them, but none comes close to finasteride or dutasteride. If a supplement promises results “just like finasteride, without the side effects,” be skeptical. One caution on the numbers below: percentages from small supplement trials cannot be compared directly with prescription-drug studies, the trial designs and sizes are worlds apart.
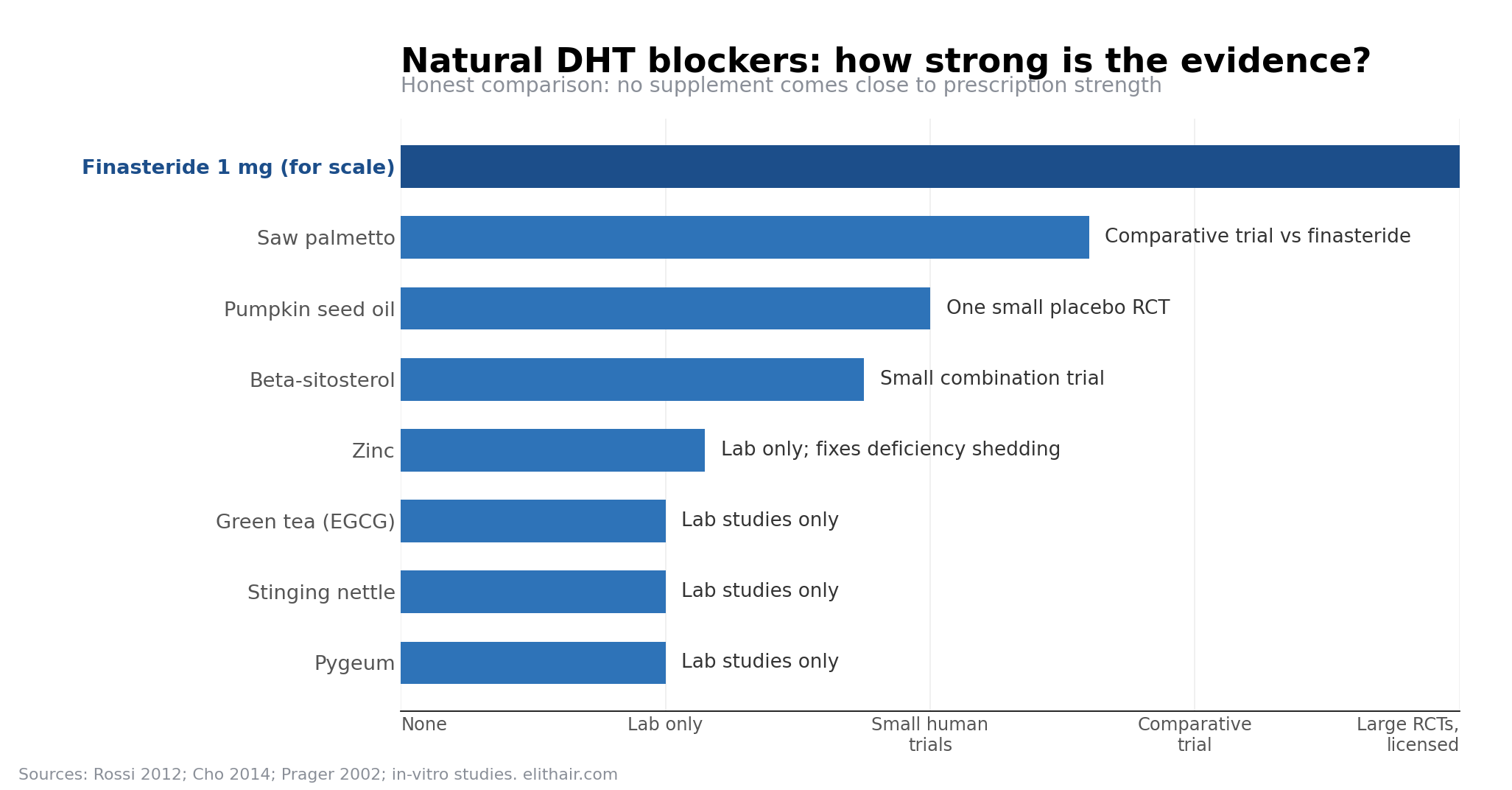
- Saw palmetto (Serenoa repens). Verdict: moderate evidence, clearly weaker than finasteride. The most studied of the bunch. It weakly inhibits both forms of 5-alpha-reductase. In the only head-to-head trial against finasteride, 38% of the saw palmetto group improved over 24 months versus 68% on finasteride, and the benefit was mostly at the crown. Better tolerated, clearly weaker.
- Pumpkin seed oil (Cucurbita pepo). Verdict: one promising small trial, mechanism unconfirmed. One Korean RCT gave men 400 mg a day for 24 weeks and saw a 40% rise in hair count versus 10% on placebo. Promising, but it is a single small trial that never actually measured DHT, so the mechanism is inferred rather than proven.
- Pygeum (Prunus africana). Verdict: plausible, unproven for hair. Contains phytosterols that inhibit 5-alpha-reductase in lab studies. Almost all the evidence comes from prostate research; there is no dedicated hair-loss trial. Plausible, unproven for hair.
- Stinging nettle (Urtica dioica). Verdict: plausible, unproven for hair. Root extracts inhibit 5-alpha-reductase in vitro and pair well with saw palmetto in prostate studies. Again, no hair-specific RCT exists.
- Beta-sitosterol. Verdict: weak, mostly lab-level evidence. A plant sterol that inhibits both forms of the enzyme in the lab. It featured in a small combination trial with saw palmetto that showed 60% improvement versus placebo, though you cannot separate which ingredient did the work.
- Zinc. Verdict: fixes deficiency-related shedding, not a true DHT blocker. A 1988 study flagged zinc as a 5-alpha-reductase inhibitor in vitro. That is 35-plus years old with no modern trial confirming it lowers scalp DHT. Where zinc genuinely helps is correcting a deficiency that causes shedding, which is nutritional, not anti-androgenic. Adequate intake is sensible; megadoses are not, since too much zinc depletes copper and upsets the gut.
- Green tea (EGCG). Verdict: lab-only, not a treatment. Inhibits Type I 5-alpha-reductase in cell cultures, but not the Type II form that drives most hair loss, and there is no quality human trial for hair. Fine as a healthy habit, not a treatment.
A quick correction on a claim that does the rounds: caffeine does not raise your DHT. That idea traces back to a single rat study, with no human evidence behind it. Drink your coffee.
Foods that act as natural 5-alpha-reductase inhibitors
A popular search, so here is a clean list. These foods contain compounds shown in lab or limited human studies to nudge 5-alpha-reductase activity downward. The effect is mild, and “foods that block DHT” oversells it, none of them produce a measurable drop in blood DHT the way a tablet does. Treat them as a sensible diet, not a cure.
- Pumpkin seeds: phytosterols (beta-sitosterol); the one food here with a supporting RCT
- Saw palmetto berries: the source of the most-studied natural extract
- Green tea, especially matcha: EGCG inhibits Type I 5-alpha-reductase in vitro
- Stinging nettle root: phytosterols with in-vitro 5-alpha-reductase activity
- Soy and flaxseed: isoflavones with weak anti-androgenic activity in the lab
- Brazil nuts and walnuts: beta-sitosterol content
- Spinach and kale: supply zinc, which supports normal enzyme regulation
- Oysters and red meat: the richest dietary zinc sources
- Turmeric: curcumin shows anti-androgenic activity in vitro
How to lower DHT naturally
If you would rather not start a prescription yet, or you want to support whatever treatment you are on, a few levers are worth pulling. None replaces medical treatment for established pattern loss, but they help build a better hormonal environment.
Eat for it. Build in the zinc-rich and phytosterol-rich foods above, and keep your diet varied rather than chasing one “miracle” item. Sort your sleep and stress, since both feed into hormone balance and chronic stress can trigger its own type of shedding. Keep your scalp healthy with a medicated shampoo like ketoconazole a couple of times a week. And if you smoke, that is one more reason to stop; it does your follicles no favors.
Be realistic about the ceiling. Lifestyle and supplements can slow things at the margins. They will not reverse genetic miniaturization that is already well under way. If you are watching your hairline move month to month, that is the signal to see a specialist rather than buy another bottle of capsules.
Comparison table: prescription vs natural vs topical
| Option | How it works | Evidence | DHT reduction | Prescription? | Key side effects |
|---|---|---|---|---|---|
| Finasteride 1 mg (oral) | Inhibits Type II 5-AR | Strong (large RCTs) | ~70% serum / ~64% scalp | Yes (licensed) | Sexual side effects in a small minority; PFS debated |
| Dutasteride 0.5 mg (oral) | Inhibits Type I + II 5-AR | Strong, but off-label for hair in US/UK | ~92–95% serum / ~51% scalp | Yes (off-label) | Similar to finasteride; very long half-life |
| Topical finasteride/dutasteride | Same drugs, scalp-targeted | Moderate, not yet fully approved | ~35% serum (finasteride) | Yes (often compounded) | Lower systemic risk; mild skin irritation |
| Ketoconazole 2% shampoo | Inhibits Type I 5-AR locally | Weak to moderate, adjunct only | Local only, no serum effect | No (OTC/Rx by strength) | Scalp dryness, irritation |
| Saw palmetto | Weak dual 5-AR inhibition | Moderate, weaker than finasteride | Not reliably quantified | No | Well tolerated; mild GI upset |
| Spironolactone (women) | Blocks androgen receptor | Moderate (off-label) | Does not lower DHT; blocks its effect | Yes (off-label) | Menstrual changes, raised potassium |
Not sure whether you need a DHT blocker, a transplant, or both? A free Elithair hair analysis looks at your pattern of loss and donor area and tells you straight. Book your free consultation.
Side effects and safety
For most men on finasteride 1 mg, the side-effect risk is low. In the registration trials, drug-related sexual side effects affected about 3.8% versus 2.1% on placebo, the difference between the two being the real attributable risk. The list includes:
- Reduced sex drive
- Erectile difficulties
- Ejaculation problems
- Breast tenderness or enlargement (rare)
- Skin rash
Most of these resolved either with continued use or after stopping. Discontinuation rates from side effects were about the same as placebo in those trials. Dutasteride has a broadly similar profile.
Two things deserve a straight answer. Post-finasteride syndrome (PFS) describes sexual, mood, and cognitive symptoms that persist after stopping the drug. It is real for a subset of users, and regulators have responded: the FDA added persistent sexual dysfunction to the label and, in 2022, agreed to list suicidal ideation as an adverse reaction. At the same time, the true incidence is genuinely unknown and contested, and there is a clear nocebo component: in one study, 44% of men told about sexual side effects reported them, versus 15% of men who were not told (the study used the 5 mg prostate dose rather than the 1 mg hair-loss dose, but the pattern is striking). So neither dismiss it nor inflate it. Talk to your doctor, and stop the drug if something feels wrong.
The other is the pregnancy warning, repeated because it is the most important safety point on this page: women of childbearing potential must not handle crushed or broken finasteride or dutasteride tablets.
One more honest point. Stop a DHT blocker and the protection stops with it. DHT levels return to baseline within months, and the hair you were holding onto resumes thinning. These drugs manage hair loss; they do not cure it.
Who are DHT blockers for?
Mostly, men with male pattern hair loss who want to slow it down or hold what they have. They are not for everyone. Skip them, or get medical clearance first, if you are under 18, planning a PSA prostate test soon (finasteride alters the result), or have allergies to the ingredients.
For women it is more complicated, and self-prescribing is a bad idea. Oral finasteride and dutasteride are not licensed for women, largely because of the pregnancy risk, and a major trial found finasteride no better than placebo in postmenopausal women. When hair loss is linked to a hormonal cause like PCOS (polycystic ovary syndrome), doctors often reach for spironolactone instead, an androgen-receptor blocker rather than a 5-alpha-reductase inhibitor. A review of seven studies found about 81% of women on spironolactone saw some improvement. Any woman considering treatment should work it through with her doctor, because the right drug depends entirely on the cause.
How long do DHT blockers take to work?
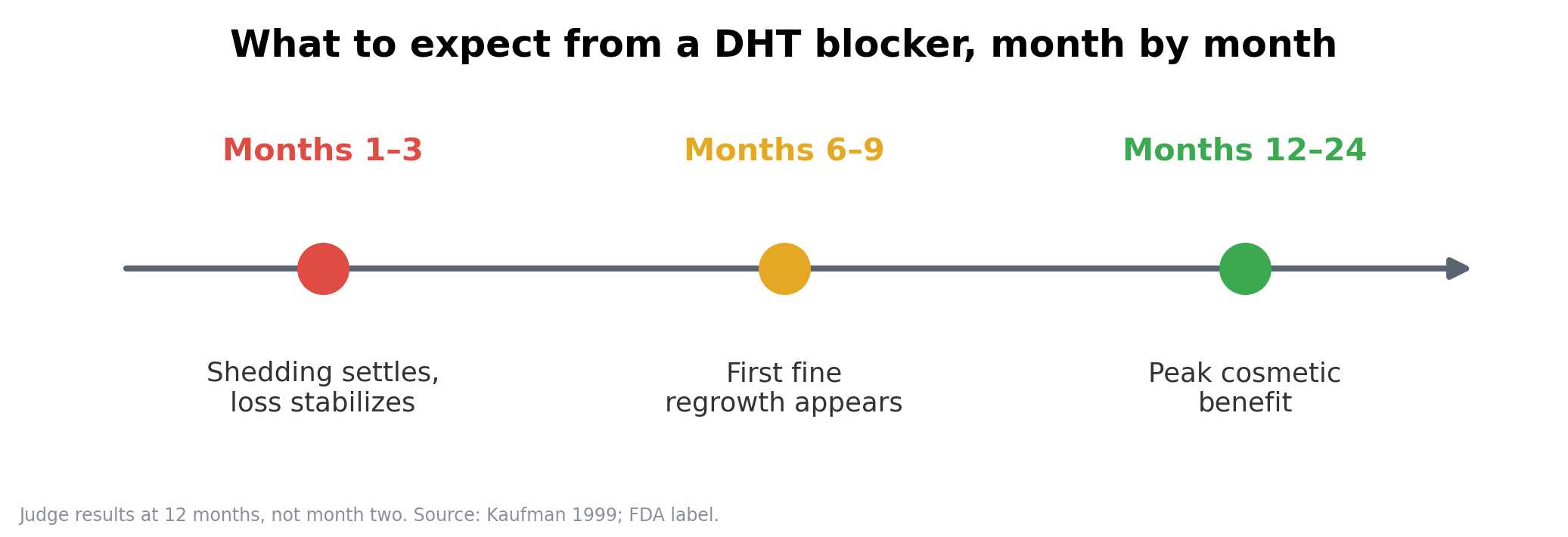
Patience is part of the deal. Hair grows slowly, so the timeline runs in months, not weeks.
In the first 3 to 6 months, the goal is stabilization. Shedding usually settles, and that alone is a win even though the mirror looks unchanged. Some men go through a brief phase of increased shedding early on, often called shock loss, as weaker hairs cycle out and stronger ones replace them. It can be unnerving, but it is generally a sign the follicles are resetting, not failing.
Around 6 to 9 months, finer regrowth starts to show. By 12 months, cosmetically meaningful regrowth is usually visible, and maximum benefit lands somewhere in the 1 to 2 year range. Keep taking it and the effect holds. Stop, and the benefit unwinds over the following year. Judge results at the one-year mark, not month two.
Do I need DHT blockers after a hair transplant?
For most patients with ongoing hair loss, the honest answer is yes, and it is good news rather than a burden.
Here is why. A transplant moves DHT-resistant follicles from the back and sides into the thinning zones. Those grafts keep their resistance, which is why transplanted hair lasts. Your native hair around the transplanted area is still genetically sensitive, though. A DHT blocker keeps that surrounding hair strong too, so the transplanted density and the rest of your hair stay in step and the whole result looks full and natural for the long run. You can see how this plays out in our hair transplant before and after results.
The evidence backs this up directly. One prospective study found men taking finasteride for 12 months after an FUE procedure had higher graft survival (94% versus 90%) and better density than men on no medication. A transplant and a DHT blocker are not rivals; they do different jobs. The surgery restores; the medication makes a strong result even stronger.
This is exactly the kind of thing worth mapping out before you commit to anything. At Elithair, the consultation looks at your hair loss pattern, your donor area, and whether ongoing medical treatment makes sense alongside a procedure, so you protect the result rather than chase it later.
Alternatives to DHT blockers
If medication is not for you, or you have reached a stage where it is no longer enough, a hair transplant is the option that restores hair permanently rather than just slowing loss. It is also worth keeping an eye on the pipeline: newer approaches like PP405 for androgenetic alopecia aim to reactivate dormant follicles, though they are still in clinical development rather than available today.
Elithair’s approach combines three stages. NEO FUE comes first, a stem-cell serum applied to the grafts before the procedure to support survival rates of up to 98%. The FUE stage is the extraction: individual grafts are removed from the DHT-resistant donor area with a micro-motor. Then DHI implantation places each graft with a Choi pen, opening the channel and setting the hair in a single step, at a natural angle and an irregular hairline so it does not look planted.
The relocated follicles keep their DHT resistance, so they do not fall out the way pattern-affected hair does. For most patients with active loss, the smart play is both: a transplant to rebuild density, and a DHT blocker to protect the native hair around it. If you are weighing up a procedure abroad, our guide to hair transplants in Turkey covers how to prepare and how to vet a clinic, and our breakdown of hair transplant costs helps you plan the budget.
You can book a free consultation and hair analysis to find out which path, medication, transplant, or both, fits your situation.
FAQ
Can DHT blockers fully stop hair loss?
They can slow loss significantly and, for some, bring back hair, but they cannot guarantee total prevention. How well they work depends on genetics, age, and how early you start. For advanced thinning, pairing a DHT blocker with a hair transplant tends to give the best overall result.
Are DHT blockers safe for long-term use?
Finasteride and dutasteride are generally considered safe long-term under medical supervision. A minority of men experience side effects such as reduced libido or erectile difficulties. Regular check-ups and your doctor’s guidance matter throughout.
Do DHT-blocker shampoos work?
Medicated shampoos like ketoconazole can support scalp health and add a mild local effect, but they cannot lower the DHT in your blood and are far weaker than oral medication. They work best as part of a broader plan, not on their own.
Can women take DHT blockers?
Some, but only under medical guidance. Oral finasteride and dutasteride are not approved for women, especially during pregnancy. For hormonal hair loss such as PCOS, doctors often prescribe spironolactone, which blocks the androgen receptor rather than reducing DHT production.
Will my hair fall out if I stop taking them?
Yes. Once you stop, DHT returns to its baseline level within months and the original hair loss process resumes. This is why many people opt for a long-term plan or a permanent solution like a hair transplant.
Can diet or lifestyle affect DHT levels?
To a degree. Foods rich in zinc and phytosterols (pumpkin seeds, green tea, leafy greens), better sleep, and lower stress all support hormone balance. The effect is mild, though, and will not reverse genetic miniaturization on its own. Despite what you may have read, normal caffeine intake does not raise DHT in humans.
Are DHT blockers effective for all types of hair loss?
No. They target androgenetic alopecia (male and female pattern loss). They do little for hair loss caused by stress, autoimmune conditions, or scarring alopecia. A proper diagnosis is the first step.
How do I know if DHT blockers are right for me?
Through a medical consultation and scalp analysis. At Elithair, specialists assess your hair, your pattern of loss, and your donor area to advise whether a DHT blocker, a transplant, or both makes sense for you.
Do DHT blockers lower testosterone or affect the gym?
Not meaningfully. They reduce DHT, not testosterone, so most men notice no change in muscle or performance. If you have specific fitness concerns, raise them with your doctor before starting.
Can I combine DHT blockers with minoxidil?
Yes, and it is one of the most common pairings. Minoxidil is not a DHT blocker; it is a vasodilator that stimulates follicles through a different mechanism. Because the two work in different ways, using them together tackles both the hormonal and the growth side of hair loss.
Medically reviewed by Dr. Imad Moustafa, hair transplant specialist.
Sources
View all sources
- Diani AR et al. (1992). The effects of finasteride on scalp skin and serum androgen levels in men with androgenetic alopecia. JAAD / ScienceDirect. Link
- Kaufman KD et al. (1999). Finasteride in the treatment of men with androgenetic alopecia. JIDSP. Link
- StatPearls NBK603726. Dutasteride pharmacology. Link
- Zhou Z et al. (2019). The efficacy and safety of dutasteride compared with finasteride in treating men with AGA: systematic review and meta-analysis. Clinical Interventions in Aging. Link
- Wikipedia. Dutasteride, regulatory history. Link
- Piraccini BM et al. (2022). Efficacy and safety of topical finasteride spray solution for male androgenetic alopecia: a phase III RCT. PMC9297965. Link
- FDA Alert (2025). Potential risks associated with compounded topical finasteride products. Link
- Adil A, Godwin M. (2019). A systematic review of topical finasteride in the treatment of androgenetic alopecia. PMC6609098. Link
- FDA Propecia Label (2022). PROPECIA (finasteride) 1 mg tablets. Link
- Multidimensional assessment of adverse events of finasteride. PLOS ONE 2024. Link
- Rossi A et al. (2012). Comparative effectiveness of finasteride vs Serenoa repens in male androgenetic alopecia: a two-year study. Int J Immunopathol Pharmacol. 25(4):1167–1173.
- Prager N et al. (2002). A randomized, double-blind, placebo-controlled trial of botanically derived inhibitors of 5-alpha-reductase in androgenetic alopecia. J Altern Complement Med. 8(2):143–152.
- Cho YH et al. (2014). Effect of pumpkin seed oil on hair growth in men with androgenetic alopecia: an RCT. Evid Based Complement Alternat Med. PMC4017725. Link
- NIH Endotext / Male Androgenetic Alopecia. NBK278957. Link
- Kaufman KD. (2002). Androgens and alopecia. Molecular and Cellular Endocrinology. Link
- Gupta AK et al. (2025). Role of topical ketoconazole in therapeutic hair care. JEADV Clinical Practice. Link
- Kessels AG et al. (2004). Ketoconazole as an adjunct to finasteride in the treatment of androgenetic alopecia. Link
- Piérard-Franchimont C et al. (1998). Ketoconazole shampoo: effect of long-term use in androgenic alopecia. Dermatology. Link
- Fields JR et al. (2020). Topical ketoconazole for the treatment of androgenetic alopecia: a systematic review. Dermatologic Therapy. Link
- In-vitro study on beta-sitosterol (2024). Inhibitory potential of phytosterols on 5-alpha-reductase activity. PMC11597715. Link
- Mondaini N, Gontero P, Giubilei G, et al. (2007). Finasteride 5 mg and sexual side effects: how many of these are related to a nocebo phenomenon? J Sex Med. 4(6):1708–1712. Link
- Rathnayake D, Sinclair R. (2023). Efficacy and safety of oral and topical spironolactone in androgenetic alopecia: a systematic review. PMC10010138. Link
- Phase II RCT topical dutasteride (2025). Safety and efficacy of dutasteride topical solution in men with AGA. PMC12405733. Link
- Kishen A, John RS, Krishnan M, Kumar S. (2025). Post operative finasteride following hair transplant compared with no medication: a prospective comparative study. J Chem Health Risks. 15(5). Link
- Messenger AG, Rundegren J. (2004). Minoxidil: mechanisms of action on hair growth. Br J Dermatol. 150(2):186. Link
- Rath M et al. (2012). Chronic caffeine intake in rat ventral prostate. PMC3521899. Link (rat study, not human evidence)
- NIH Bookshelf NBK278957 / ISHRS clinical practice. Donor dominance and native-hair miniaturization. Link
- Liao S, Hiipakka RA. (1995). Selective inhibition of steroid 5-alpha-reductase isozymes by tea epicatechin-3-gallate and epigallocatechin-3-gallate. Biochem Biophys Res Commun. 214(3):833–838. Link. And Kwon OS et al. (2007). Human hair growth enhancement in vitro by green tea EGCG. Phytomedicine. 14(7-8):551–555. Link (both in-vitro)
- Stamatiadis D et al. (1988). Inhibition of 5-alpha-reductase activity in human skin by zinc and azelaic acid. Br J Dermatol. Link

Dr. Imad Moustafa
Hair transplant specialist