
In brief: corticosteroids for hair loss
Glucocorticoids (commonly called cortisone, technically corticosteroids) are anti-inflammatory steroid hormones produced by the adrenal cortex. For hair loss, they only work where inflammation or a misdirected immune reaction is attacking the hair follicle. Cortisone is not a general hair-growth product, and in any effective strength it is prescription-only.
- Where cortisone helps: alopecia areata (patchy hair loss), scarring alopecias (lichen planopilaris, frontal fibrosing alopecia), inflamed scalp conditions (scalp psoriasis, seborrheic dermatitis).
- Where cortisone does not help: hereditary androgenetic hair loss, as well as diffuse hair loss caused by iron deficiency, thyroid issues or stress.
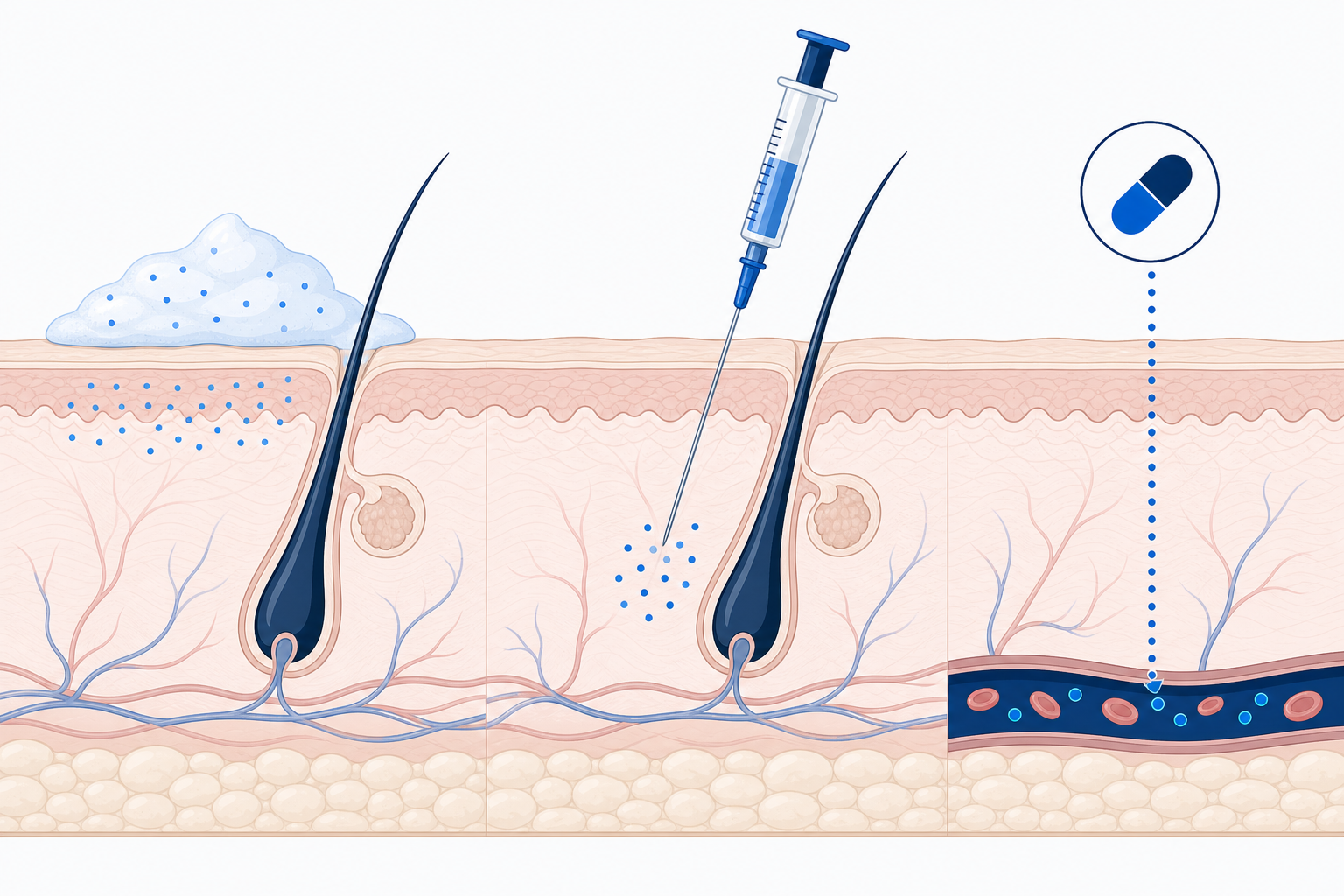
- Forms: topical (ointment, solution, foam), intralesional injection (triamcinolone into the bald patch), systemic (tablets). The choice depends on the diagnosis and severity.
- Important: prescription-only, used only under dermatological supervision. The type of hair loss you have determines whether it can work.
Many people search for “cortisone for hair loss” hoping for a remedy that slows down any kind of hair loss. That expectation is often misleading. Glucocorticoids treat inflammation at the hair follicle, not “hair loss in general.” This article explains which causes cortisone actually works on, the forms in which it is used, the side effects it carries and why the diagnosis always belongs in the hands of a dermatologist. Information current as of June 2026, with reference to the current S3 guideline on alopecia areata (AWMF 013-104, published 23 February 2026).
Summary
- What are glucocorticoids (cortisone, corticosteroids)?
- Cortisone for hair loss: when it really helps (and when it does not)
- Alopecia areata: the main reason cortisone is prescribed
- Cortisone ointment, solution and foam (topical glucocorticoids)
- Cortisone injection (intralesional injection)
- Cortisone tablets (systemic glucocorticoids)
- Use in scarring alopecia and scalp inflammation
- Prescription requirement, self-medication and “cortisone without a prescription”
- Cortisone for hair loss: how quickly does it work? (regrowth timeline)
- Can cortisone itself cause hair loss?
- When the hair loss is stable: is a hair transplant an option?
- When you should see a dermatologist about hair loss
- Frequently asked questions about glucocorticoids (cortisone) in hair loss
- Sources
What are glucocorticoids (cortisone, corticosteroids)?
Glucocorticoids (commonly called cortisone) are steroid hormones produced by the adrenal cortex, either occurring naturally in the body or synthetically reproduced. In hair loss, they dampen misdirected immune reactions and inflammation directly at the hair follicle. According to the Gelbe Liste, they have a “pronounced anti-inflammatory and immunosuppressive effect.” They are the anti-inflammatory subgroup of the corticosteroids, and “cortisone” is the everyday umbrella term for this group of active substances.
To clarify the terminology: corticosteroids are the broad term for steroid hormones of the adrenal cortex, while glucocorticoids are the anti-inflammatory subgroup. Synthetic examples include prednisolone, dexamethasone, betamethasone, triamcinolone and clobetasol. In everyday use “cortisone,” “corticosteroids” and “glucocorticoids” are treated as largely interchangeable, which is why this article uses them as synonyms.
How glucocorticoids act on the hair follicle
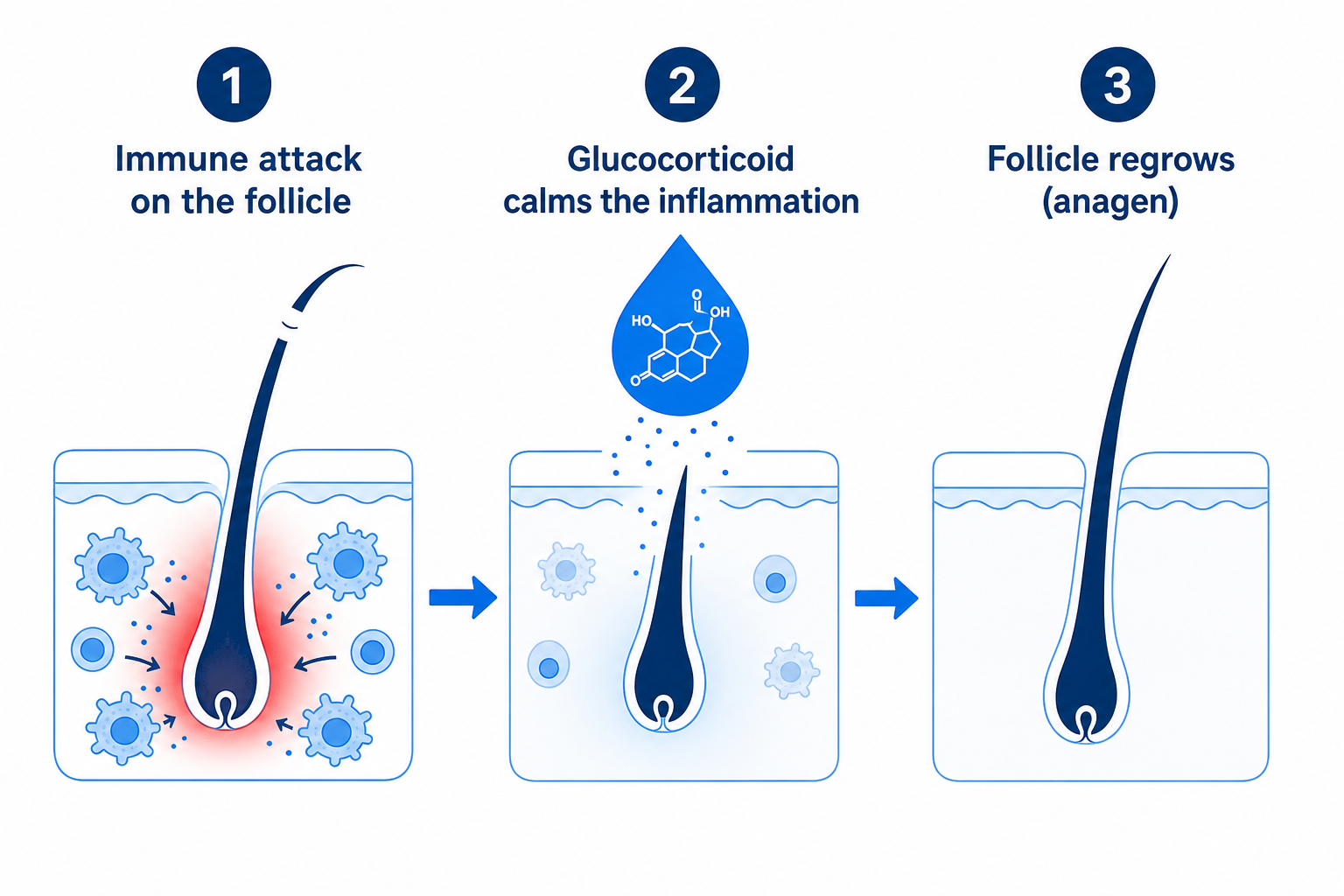
Glucocorticoids act on the hair follicle by curbing the inflammatory attack of immune cells. They bind intracellularly to glucocorticoid receptors, inhibit pro-inflammatory messenger substances and thereby reduce the reaction against the follicle. According to a review in PMC (PMC5939003), the mechanism of topical corticosteroids consists of “containing the inflammation and accelerating the recovery of damaged hair follicles.”
Crucial for managing expectations: when the immune attack is dampened, the follicle can re-enter the growth phase (anagen) from the resting phase. We explain the logic of the resting and growth phases in detail in our article on the hair cycle. Cortisone therefore treats the inflammation, not a genetic or nutritional cause.
Cortisone for hair loss: when it really helps (and when it does not)
Cortisone for hair loss only helps when the hair loss is caused by inflammation or autoimmunity. In the most common type, hereditary androgenetic hair loss, it is ineffective, because there is no inflammatory process there but rather a genetically driven sensitivity of the follicles to the hormone DHT. Diffuse hair loss caused by iron deficiency, thyroid problems or stress also does not respond to corticosteroids.
If you have hereditary (androgenetic) hair loss, the evidence-based routes are not corticosteroids but minoxidil, finasteride or, with a suitable diagnosis, a hair transplant. Cortisone would find no mechanism to act on here. The dermatological diagnosis determines which type you have.
The most important inflammatory indication is alopecia areata (patchy hair loss). According to the Rochester Epidemiology Project, its lifetime prevalence is around 2.1 percent, meaning roughly two in a hundred people over the course of their lives. In Germany, around 170,000 people are affected according to the S3 guideline (Charité, 2026). The table below classifies the most common types of hair loss.
| Type of hair loss | How to recognize typical symptoms | Cause | Inflammatory/autoimmune? | Cortisone useful? | Typical treatment |
|---|---|---|---|---|---|
| Alopecia areata (patchy hair loss) | Sudden, sharply defined round bald patches, scalp otherwise unremarkable | Autoimmune, the immune system attacks the follicle | Yes | Yes, first-line depending on extent | Topical, intralesional injection, possibly systemic, JAK inhibitors |
| Scarring alopecia (lichen planopilaris, FFA) | Shiny, scarred-looking bald areas with no visible follicle openings, often redness/itching at the edges | Inflammatory and scarring | Yes | Yes, to slow the progression | High-potency topicals, intralesional, systemic, dermatological |
| Scalp psoriasis (psoriasis capitis) | Thick, silvery-white scales on reddened scalp, accompanied by hair loss | Inflammatory | Yes | Yes, treats the underlying condition | Topical corticosteroid class III/IV, often with a vitamin D analog |
| Seborrheic dermatitis of the scalp | Greasy, yellowish scales, reddened, itchy scalp | Inflammatory | Partly | Yes, as a supportive measure | Mild corticosteroids plus antifungals as the main therapy |
| Androgenetic (hereditary) hair loss | Slowly progressing receding hairline, thinning crown/parting, no inflammation | Genetics, DHT sensitivity | No | No, ineffective | Minoxidil, finasteride, possibly a hair transplant |
| Diffuse/telogen hair loss (iron, thyroid, stress) | Even thinning across the whole head, increased hair loss when washing/combing | Nutrient/hormone deficiency | No | No, address the cause | Supplementation, watchful waiting, recovery once the cause is corrected |
This distinction is the heart of the matter: corticosteroids for hair loss are highly effective for the right cause and ineffective for the wrong one. If you have diffuse shedding caused by iron deficiency or the thyroid, the cause should be treated, not the follicle dampened with cortisone.
Alopecia areata: the main reason cortisone is prescribed
Alopecia areata (patchy hair loss) is an autoimmune condition in which the immune system attacks the hair follicles. Glucocorticoids are one of the established first-line therapies here. The typical sign is sharply defined, round bald patches. Importantly, the follicles remain intact, which is why the hair loss is generally reversible, unlike with scarring alopecias.

Cortisone dampens the immune attack locally or systemically so that the follicle can recover. The current S3 guideline on alopecia areata (AWMF register 013-104, published 23 February 2026, Charité Berlin) lists topical corticosteroids, intralesional injection and systemic therapy as established treatment strategies with long-standing evidence. The guideline comprises 79 evidence- and consensus-based recommendations.
To be honest about it: in mild forms, spontaneous recovery is common. According to a review (PMC10072216), patients with under 25 percent scalp involvement show spontaneous regression in up to 68 percent of cases, while with more than 50 percent involvement this drops to around 8 percent. More recent placebo-controlled studies, however, estimate spontaneous remission more cautiously. The course is highly variable and should be assessed by a dermatologist.
As a newer alternative for severe alopecia areata, JAK inhibitors such as baricitinib (EU approval 2022) and ritlecitinib (EMA approval 2023) are approved. They are currently not reimbursed by the statutory health insurance in Germany. Whether they are an option is decided solely by the treating dermatologist.
Cortisone ointment, solution and foam (topical glucocorticoids)
Topical glucocorticoids are ointments, solutions or foams containing cortisone that are applied directly to the scalp. They are usually the first step for limited inflammatory hair loss. They are classified by potency into four strength classes (Niedner classification, Germany), from class I (weak, e.g. hydrocortisone) to class IV (very strong, e.g. clobetasol propionate).
In alopecia areata, high-potency active substances are usually used, such as clobetasol propionate 0.05 percent (class IV) or mometasone furoate 0.1 percent (class III). In a study of 34 patients over 12 to 24 weeks, 89 percent responded with regrowth (clobetasol foam, haarerkrankungen.de). Another study with a clobetasol ointment found a satisfactory response in only around 18 percent. The range depends heavily on the severity.
On the common “ointment or solution” question: on the hair-bearing scalp, solutions, foams or tinctures are usually prescribed instead of greasy ointments. They are easier to apply between the hairs and penetrate better. A glucocorticoid ointment in the classic sense is rather impractical on the scalp, but the mechanism of action remains the same.
Local side effects of topical corticosteroids are rare with proper, limited use. With overly long or overly strong use, there is a risk of skin atrophy (skin thinning), telangiectasia (dilated fine blood vessels), steroid acne or pigmentation disorders (PharmaWiki). The scalp, however, is considered a relatively resilient zone with a lower atrophy risk than other parts of the body.
Important note on self-treatment: Weak, over-the-counter hydrocortisone creams (class I) from the medicine cabinet are not intended for treating hair loss and are not effective for this use. Using them without a diagnosis mainly risks delaying treatment of the actual cause. An effective topical glucocorticoid ointment or solution belongs in a doctor’s prescription.
Cortisone injection (intralesional injection)
A cortisone injection for the hair is an intralesional injection, usually with triamcinolone acetonide, directly into the bald patch on the scalp. It is regarded as the standard therapy for limited alopecia areata in adults. A concentration of around 5 mg/ml is common on the scalp, with a guideline maximum of about 20 mg per session (springermedizin.at).
Procedure: the dermatologist makes several small injections per bald area with a fine needle. The sessions are typically repeated every 4 to 6 weeks (PMC3002419), often in a series of three to five appointments. The injection is usually well tolerated and only mildly stinging. This method cannot be self-administered.
On the effect: a first response typically appears in studies after 4 to 8 weeks (PMC3002419). The response rates vary with the concentration. In clinical studies, hair growth at around 5 mg/ml was approximately 80 percent, lower at lower concentrations. Higher concentrations brought no advantage, only more side effects. If no improvement appears after about 6 months, the therapy is reconsidered.
Local side effects of the cortisone injection are temporary dimples (skin atrophy at the injection site), hypopigmentation (lightening) and telangiectasia. According to the literature (PMC3002419), these usually resolve on their own. It is precisely this targeted, local potency that is the advantage of the injection over ointment treatment alone.
Cortisone tablets (systemic glucocorticoids)
Systemic glucocorticoids (cortisone tablets or infusions) are used only for severe, rapidly progressing or extensive forms, because they affect the entire body. Typical reasons are rapidly progressive or extensive alopecia areata, up to alopecia totalis or universalis. Usually a time-limited burst (pulse therapy) is given, not a long-term therapy.
The effect sets in quickly, but the risk of relapse after stopping is high. In studies, the response rate in multifocal alopecia areata was around 50 percent after 6 months, considerably lower in alopecia totalis or universalis (Karger). This is precisely why doctors carefully weigh the benefit against the side effects.
The systemic side effects must be taken seriously: weight gain and fat redistribution (a Cushing-like picture), elevated blood pressure, elevated blood sugar (up to a fourfold higher diabetes risk according to medicoconsult.de), psychological changes, increased susceptibility to infection and stomach complaints. With prolonged use, osteoporosis and a suppression of the body’s own adrenal function are added.
Contraindications: when cortisone is not used or only with restrictions
Whether cortisone may be used for hair loss is assessed by the doctor on a case-by-case basis, because there are situations in which particular caution or avoidance is warranted. Since all effective corticosteroids are prescription-only, this weighing-up is always done by a doctor. Relevant pre-existing conditions such as poorly controlled diabetes, high blood pressure, osteoporosis, gastrointestinal ulcers or active infections may argue against systemic therapy.
During pregnancy and breastfeeding, a particularly strict benefit-risk assessment applies. The treatment of hair loss, which is cosmetically motivated in any case, then usually takes a back seat, and the doctor decides whether, in what form and at what dose any treatment is given at all. Self-medication with cortisone is not indicated during this time. Which therapy is appropriate should be clarified exclusively with the treating physician.
Never stop on your own: Systemic glucocorticoids suppress the body’s own adrenal function (the HPA axis), which can already be disrupted after around two weeks of higher dosing. Abruptly stopping could trigger adrenal insufficiency. The dose is therefore reduced exclusively by a doctor and step by step. With prolonged systemic therapy, the doctor may additionally consider bone-protective accompanying therapy (e.g. calcium and vitamin D).
Use in scarring alopecia and scalp inflammation
In scarring (cicatricial) alopecias such as lichen planopilaris or frontal fibrosing alopecia, cortisone is meant to stop the inflammation before follicles are permanently destroyed. Here lies an important difference from alopecia areata: follicles that are already scarred no longer grow back (universimed.ch). The goal is therefore to stop the progression, not to regenerate hair.
High-potency topical corticosteroids and intralesional triamcinolone injections are used, and in active progression also systemic therapy. Because every new flare of inflammation can irreversibly destroy follicles, an early start of therapy is decisive. Anyone who notices shiny, scarred-looking bald areas with no visible follicle openings should see a dermatologist promptly.
Inflammatory scalp conditions that secondarily promote hair loss are also treated with cortisone. In scalp psoriasis, topical corticosteroids of class III/IV are first-line, often combined with a vitamin D analog. In seborrheic dermatitis, mild corticosteroids together with antifungals are used as the main therapy. Once the underlying condition heals, the accompanying hair loss usually recedes.
Prescription requirement, self-medication and “cortisone without a prescription”
Glucocorticoids for hair loss are prescription-only in any effective strength. This applies to topical corticosteroids of classes II to IV as well as to all intralesional injections and systemic tablets. Only weak hydrocortisone preparations (up to about 0.5 percent) for mild eczema and itching are available over the counter, and these are not intended for hair loss.
“Cortisone for hair loss without a prescription” is therefore not a sensible option. Without a diagnosis, there is a risk of the wrong therapy, of masking the findings and of unnecessary side effects. According to the Pharmazeutische Zeitung, the most important recommendation is therefore: first clarify the cause with a dermatologist, then treat it specifically. A sound diagnosis often begins with the patient history and, if appropriate, a blood test for hair loss.
On the cost question: with a confirmed medical indication, such as diagnosed alopecia areata, topical corticosteroids and intralesional injections are generally covered by the statutory health insurance. JAK inhibitors, by contrast, are currently not reimbursed. The details are clarified by the treating practice.
| Form | How it is used | Typical use | Advantages | Side effects/notes |
|---|---|---|---|---|
| Topical (solution, foam, tincture) | Applied to the scalp, 1 to 2 times daily | Limited inflammatory hair loss, first step | Fewer side effects, can be used at home | Skin atrophy with overuse; prescription-only in any effective strength |
| Intralesional injection (triamcinolone) | Injection into the bald patch, every 4 to 6 weeks | Limited alopecia areata in adults | High local potency, targeted | Temporary dimples/lightening (usually reversible); only at the doctor’s office |
| Systemic (tablets/infusion) | Oral (prednisolone) or intravenous | Severe, rapid or extensive forms | Acts on the whole body, quickly | Weight, blood pressure/sugar, osteoporosis, adrenal suppression; relapse after stopping is common |
Cortisone for hair loss: how quickly does it work? (regrowth timeline)
With a responsive, inflammatory cause, cortisone for hair loss shows first effects after weeks, while visible regrowth follows over months in line with the natural hair cycle. A first response to the intralesional injection can be expected after 4 to 8 weeks according to PMC3002419, and after about 6 to 14 weeks with topical use. The following timeline shows the realistic course.
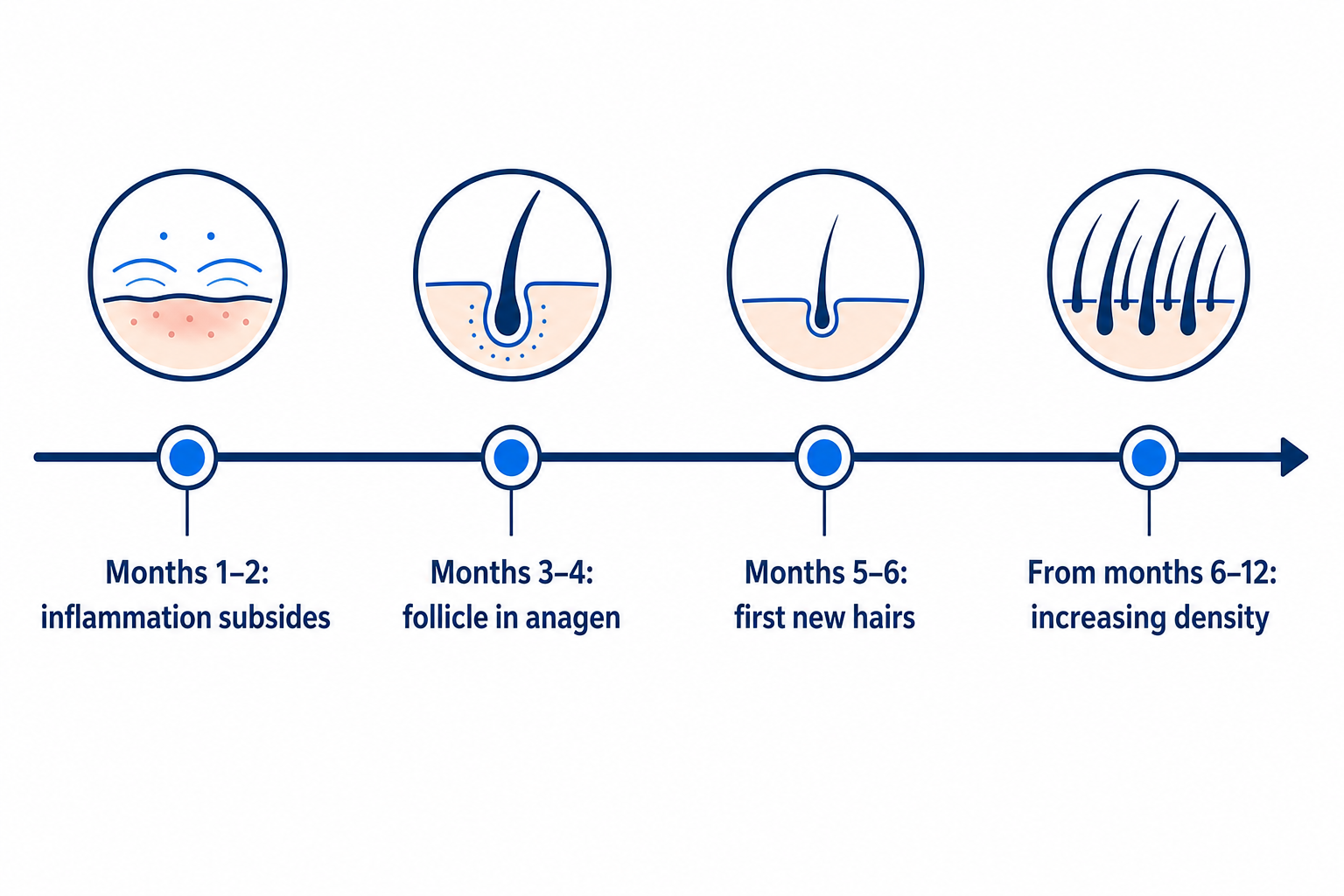
| Point in time | What happens in the follicle | What you notice |
|---|---|---|
| Months 1 to 2 | Inflammation and immune attack subside | Hair loss slows, then stops; scalp calms down |
| Months 3 to 4 | Follicles re-enter the growth phase (anagen) | Still little visible, first fine hairs palpable |
| Months 5 to 6 | New hair grows in, often thin and lighter at first | First new hairs visible, partly depigmented |
| From months 6 to 12 | Hair normalizes in thickness and pigmentation | Increasing density, color often returns |
An honest classification is part of the picture: a relapse after stopping is common. After systemic cortisone therapy, alopecia areata recurs in around 60 percent of cases (haarerkrankungen.de, springermedizin.at). This reflects the chronic, relapsing course of the condition, not a failure of the therapy. Cortisone suppresses the immune attack while it is active, but it does not eliminate the autoimmune predisposition.
Can cortisone itself cause hair loss?
Cortisone is used against hair loss, but in rare cases, especially with high-dose long-term use, it can itself contribute to diffuse hair loss. With long-term systemic therapy, metabolic and hormonal effects can trigger a premature transition of follicles into the resting phase, that is, a telogen effluvium (blog.hairsystems-heydecke.de). This shedding is usually reversible.
This is not a contradiction but a distinction: the targeted treatment of an inflammatory cause differs from the unwanted effect of a long, high-dose systemic therapy. With short-term or topical use and a correct indication, this effect is not a relevant problem. If new hair loss occurs during ongoing cortisone therapy, the rule is: talk to the treating doctor, do not stop on your own.
When the hair loss is stable: is a hair transplant an option?
A hair transplant is explicitly not indicated for active inflammatory or autoimmune hair loss. In active alopecia areata it is contraindicated, because the immune system would attack transplanted follicles as well. The same applies to active scarring alopecias as long as the inflammation is progressing. Here dermatological treatment comes first, not a procedure.
Only with a demonstrably stable, burnt-out condition, such as a long-quiescent scarring alopecia after dermatological confirmation of inactivity (often after at least one year of inactivity), can a hair transplant even be considered. The classic transplant case, by contrast, is hereditary androgenetic hair loss, an entirely different, non-inflammatory cause. Often more than one type is even present at the same time.
Which form of hair loss you have, and whether a procedure makes sense at all, is first clarified by the dermatological diagnosis. A non-binding hair analysis at Elithair examines the visual distribution pattern and can help to differentiate the hair type. It does not replace a medical blood test or a dermatological diagnosis of the underlying condition, but is a first, advisory filter.
Perspective from the Elithair consultation
“In our consultations we regularly meet people with patchy hair loss who ask whether a hair transplant would be the fastest solution. As long as the inflammation is active, that would be a mistake, because the immune system would attack the transplanted follicles just the same. Our work begins with a careful distinction: is there an inflammatory hair loss that belongs in dermatological treatment? Or is there additionally a genetic hair loss that responds to a transplant independently of that? This distinction protects those affected and builds genuine trust.”
Elithair Medical Board
When you should see a dermatologist about hair loss
Whether cortisone is an option for hair loss depends solely on the diagnosis. The following warning signs point to an inflammatory or autoimmune cause and should be clarified by a dermatologist promptly. With scarring forms, every week counts, because destroyed follicles do not return.
Sudden, round, sharply defined bald patches point to alopecia areata.
An itchy, reddened, flaky or painful scalp with hair loss points to an inflammatory cause.
Scarred or shiny-looking bald areas with no visible follicle openings need urgent clarification (suspected scarring alopecia).
Rapid, widespread hair loss within a few weeks should be examined by a doctor.
Always discuss hair loss during ongoing cortisone therapy with your doctor, do not stop on your own.
For background on the various triggers, it is worth looking at the causes of hair loss. Women with diffuse thinning will find further context in the article on hair loss in women.
Frequently asked questions about glucocorticoids (cortisone) in hair loss
Does cortisone help against hair loss?
Yes, but only for hair loss caused by inflammation or autoimmunity, above all alopecia areata. For genetic-androgenetic or nutrient-related diffuse hair loss, cortisone is ineffective.
For which type of hair loss does cortisone work?
For alopecia areata (patchy hair loss), scarring alopecias (lichen planopilaris, FFA) and inflammatory scalp conditions such as scalp psoriasis or seborrheic dermatitis. Not for androgenetic or diffuse deficiency-related hair loss.
What is the difference between cortisone ointment, injection and tablets?
An ointment or solution (topical) is applied to the scalp and is the first step for limited hair loss. The injection (intralesional) works directly and strongly in the bald patch. Tablets (systemic) are used for severe forms, act on the whole body and have more side effects.
How quickly does cortisone work against hair loss?
First signs of a response usually appear after 4 to 14 weeks. Visible regrowth typically follows from month 3 to 6, because the hair cycle follows this pace.
Does hair grow back after cortisone?
With alopecia areata, yes, because the follicles remain intact and re-enter the growth phase when the treatment responds. With scarring alopecias, follicles that are already destroyed do not grow back; here the aim is to stop the progression.
Does hair fall out again after stopping cortisone?
With alopecia areata this is common. In studies, around 60 percent of patients experienced a relapse after stopping. This is due to the chronic, relapsing course of the condition, not to a failure of the therapy.
What side effects does cortisone have in hair loss?
Local (topical or injection): skin atrophy, telangiectasia and temporary dimples, usually reversible. Systemic (tablets): weight gain, elevated blood pressure and blood sugar, osteoporosis, adrenal suppression and increased susceptibility to infection.
Is cortisone for hair loss prescription-only?
Yes. All therapeutically effective corticosteroids (topical class II to IV as well as all intralesional and systemic forms) are prescription-only. Weak, over-the-counter hydrocortisone creams are not a therapy against hair loss.
Does cortisone help with hereditary (androgenetic) hair loss?
No. Androgenetic hair loss is not an inflammatory process, so cortisone has no mechanism to act on there. Effective options are minoxidil, finasteride or, with a suitable diagnosis, a hair transplant.
Can cortisone itself cause hair loss?
In rare cases, high-dose, long-term systemic use can promote a diffuse telogen hair loss. This is usually reversible after reducing the dose or stopping. With short-term or topical use it is not a relevant problem.
Can I have a hair transplant after inflammatory hair loss has healed?
Only after a demonstrably stable, burnt-out condition and after dermatological confirmation of inactivity. With active disease, a hair transplant is contraindicated. An accurate diagnosis is always the first step.
Sources
- AWMF S3 guideline “Diagnostik und Therapie der Alopecia areata,” no. 013-104, published 23 February 2026, Charité Berlin. register.awmf.org
- Fan, Dang, Srivastava: Intralesional Steroids for Alopecia Areata, 2010, PMC3002419. pmc.ncbi.nlm.nih.gov
- Pratt et al.: Alopecia Areata, Burden of Disease and Treatment, PMC10072216. pmc.ncbi.nlm.nih.gov
- Strazzulla et al.: Alopecia Areata, Review of Epidemiology and Treatment Options, PMC5939003. pmc.ncbi.nlm.nih.gov
- Corticosteroid pulse therapy in alopecia areata, 10-year results, Kompass Dermatologie (Karger). karger.com
- Gelbe Liste, active substance group glucocorticoids. gelbe-liste.de
- PharmaWiki, topical glucocorticoids (potency classes). pharmawiki.ch
- Springermedizin, new treatment options for alopecia areata. springermedizin.at
- Universimed, lichen planopilaris and frontal fibrosing alopecia. universimed.com
- Pharmazeutische Zeitung, over-the-counter products for hair loss. pharmazeutische-zeitung.de
Note: This article is for general information and does not replace medical advice, diagnosis or treatment. Glucocorticoids are prescription-only in any effective strength. The diagnosis and treatment of inflammatory hair loss belong in the hands of a dermatologist. As of: June 2026.

Dr. Imad Moustafa
Hair transplant specialist